Authors Robin Monotti


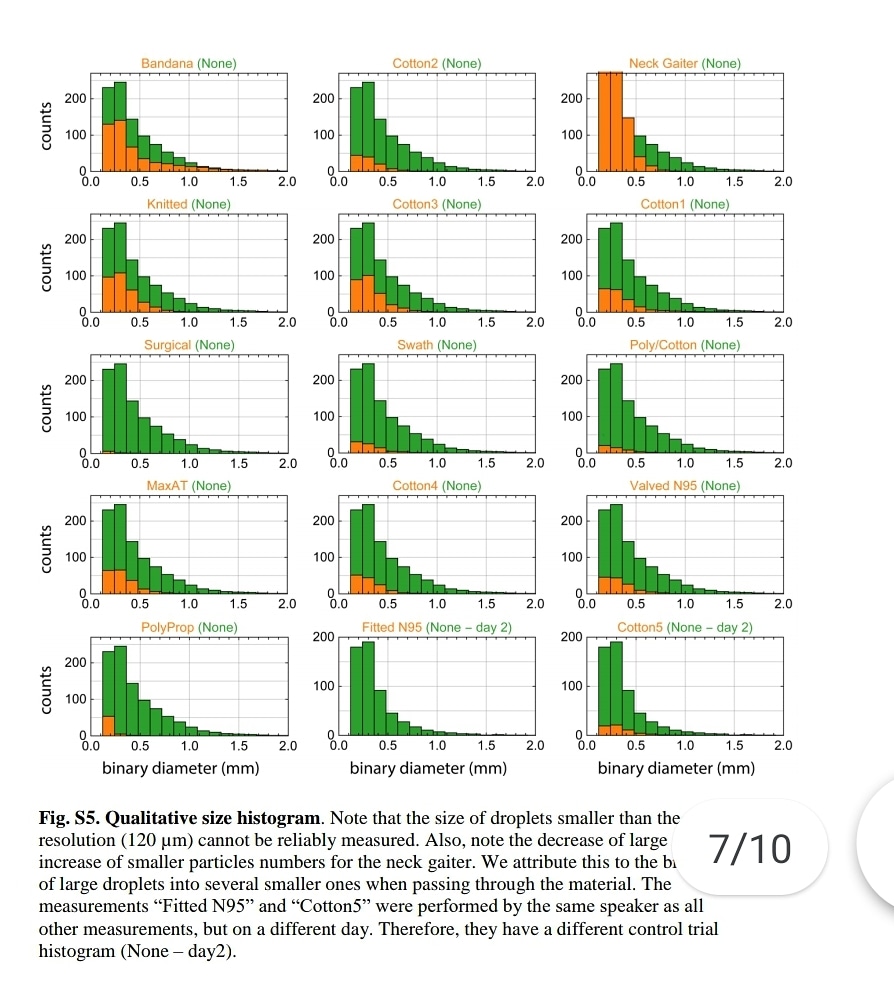
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."
https://t.co/jBQlWRxcEL
Influenza like illness rates 3 times higher with cloth masks when compared to control group:
https://t.co/djT0mfutv9
Prof. Carl Heneghan, Oxford University: "The high quality trial evidence for cloth masks suggest they increase your rate of reinfection."

Please note, droplets smaller than 120 microns can't be measured. SARSCoV2 is 0.14 microns. This means that the nebulization effect of medical masks could not be measured, not that it does not happen. ⬇️
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."https://t.co/jBQlWRxcEL pic.twitter.com/XeKYFmjsGs
— Robin Monotti (@robinmonotti) January 15, 2021
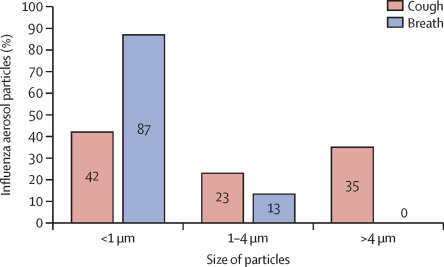
The really small aerosols <1 μm [the ones that pass through ALL surgical masks] can penetrate all the way to the alveoli - the basic units for gas exchange
4/In humans, larger aerosols deposit in upper throat, nose, & tracheobronchial region of the lung. Medium-sized aerosols mostly deposit in small airways further down. The really small aerosols <1 \u03bcm can penetrate all the way to the alveoli - the basic units for gas exchange. 4/7 pic.twitter.com/9ZJb4JrZqI
— Dr. Ali Nouri (@AliNouriPhD) December 29, 2020
Lockdowns increase infections because they lower immunity & therefore increase the disease. After hospitals & care homes households account for the largest number of transmissions. Schools/universities act as a break in transmission of the disease. All evidence based.
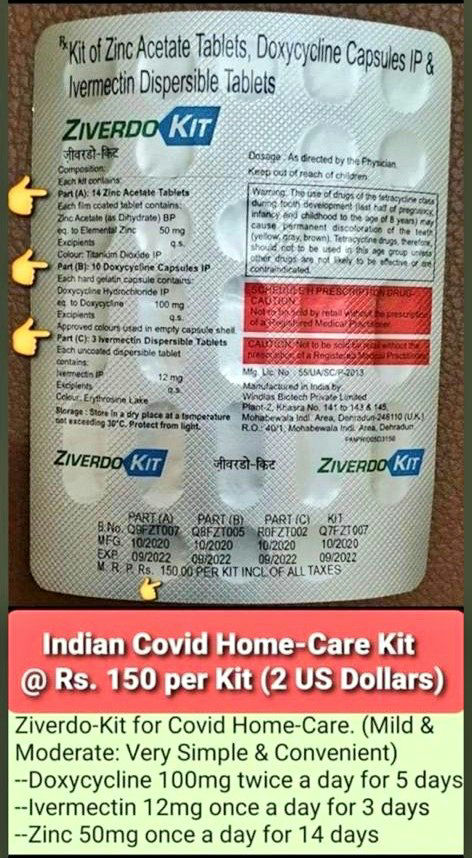
Transmission does not mean infection. I can transmit SARSCoV2 but I can't transmit Covid19. Whether SARSCoV2 develops at all into mild or severe Covid19 depends entirely on the immune system of the recipient. Early treatment prevents severe Covid19, the right treatment cures it.
"Children act more as a brake on infection," said Prof. Reinhard Berner, the head of pediatric medicine at Dresden University Hospital and leader of the study. "Not every infection that reaches them is passed
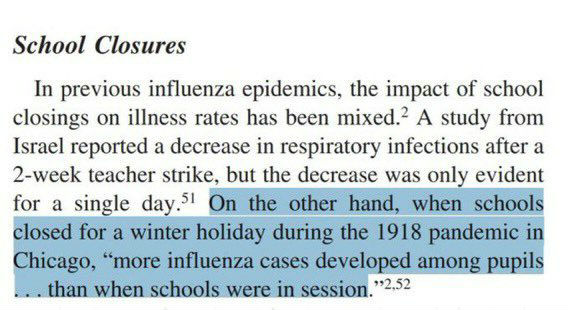
Closing schools increases transmission of respiratory viral infection because children act as a break on the community transmission of the virus. We have known this since 1918:
https://t.co/TPRYQ1LAAJ
On the 19th March 2020 the WHO released this guidance intended for healthcare workers (HCWs), healthcare managers and IPC teams at the facility level & at national and district/provincial level:https://t.co/C4aV2BnMPj pic.twitter.com/tCk1EyLskV
— Robin Monotti (@robinmonotti) December 21, 2020
It clearly does indicate both the risks of bacterial infection & to prescribe broad spectrum antibiotics as part of treatment:
"Collect blood cultures for bacteria that cause pneumonia and sepsis, ideally before antimicrobial therapy. DO NOT
delay antimicrobial therapy"
"6. Management of severe COVID-19: treatment of co-infections
Give empiric antimicrobials [broad spectrum antibiotics] to treat all likely pathogens causing SARI and sepsis as soon as possible, within 1 hour
of initial assessment for patients with sepsis."
"Empiric antibiotic treatment should be based on the clinical diagnosis (community-acquired
pneumonia, health care-associated pneumonia [if infection was acquired in health care setting] or sepsis), local epidemiology &
susceptibility data, and national treatment guidelines"
"When there is ongoing local circulation of seasonal influenza, empiric therapy with a neuraminidase inhibitor [anti-viral influenza drugs] should
be considered for the treatment for patients with influenza or at risk for severe disease."
#BMJResearch update: Corticosteroids probably reduce mortality and mechanical ventilation in patients with covid-19 compared with standard care, whereas azithromycin, hydroxychloroquine, interferon-beta, and tocilizumab may not reduce either https://t.co/oQ3lTWUqaz
— The BMJ (@bmj_latest) December 18, 2020
This meta-analysis of controlled trials only looks at hospitalized patients. How long were the patients ill for before being hospitalized? One week? Two? Three? Too late for zinc ionophores (HCQ) (+ZINC? No zinc no point..) to work. Severe illness becomes bacterial in nature.
Was azythromycin administered when the bacterial infections were also too advanced? I have seen Azythromycin work with my very own eyes but that's not to say that if administered too late it may not save the patient. How many patients were given AZT & ventilated? It's all timing.
All the meta-analysis is telling us is if you leave it too late you may have missed the early window for antiviral zinc treatment (Zn+HCQ) & that if you are given AZT when you are ventilated or very severe it may too late for it to save you & corticosteroids may be last resort.
And of course antibiotics need also probiotics, or they may harm the bacterial flora which is part of the immune response. Difficult to tell from a meta-analysis how this problem was managed.
Here is the Italian-EU scientific study indicating SARSCoV2 replicates in bacteria, not only human cells, and that is why antibiotics work and these vaccines will not:
"The preliminary results suggest that SARS-CoV-2 replicates in bacterial
2 of the 4 authors of the study work at the European Commission. Another works at an Italian medical research facility called Craniomed: https://t.co/EETSM3nb3T
You can find all of CRANIOMED's Carlo Brogna's published scientific research articles here, take a look:
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
Trust us not to turn over data. Trust us not to read your messages. Trust us not to close your channel. Maybe @Durov is an angel. I hope so! But angels have fallen before. Telegram should have been working to make channels decentralized\u2014meaning outside their control\u2014for years.
— Edward Snowden (@Snowden) December 30, 2017