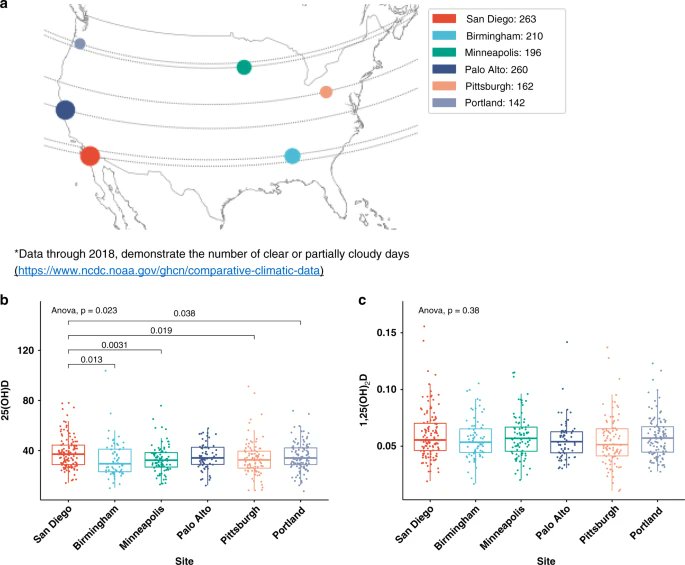
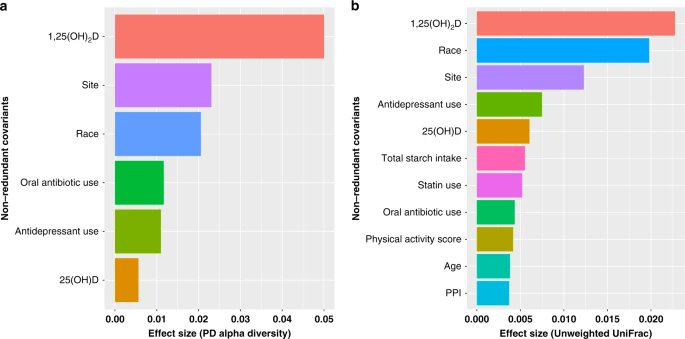
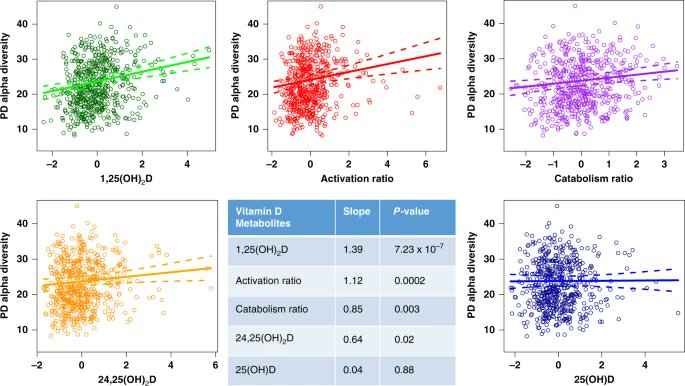
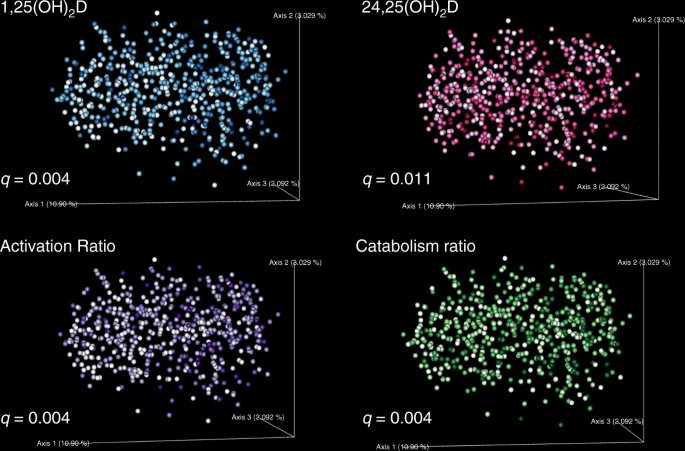
PROBIOTICS & VIT D: "The vitamin D receptor is highly expressed in the gastrointestinal tract where it transacts gene expression..These results support the underlying hypothesis that the human gut microbiome and vitamin D metabolism are integrally related"
https://t.co/15rVFa1fkk
More from Robin Monotti FRSA ⭐
Twitter removed 800 followers from my account today. People have been writing saying twitter automatically unfollowed me for them. Follow me on Parler @robinmonotti & Telegram https://t.co/o5rFaSrCpa to bypass this.
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
Trust us not to turn over data. Trust us not to read your messages. Trust us not to close your channel. Maybe @Durov is an angel. I hope so! But angels have fallen before. Telegram should have been working to make channels decentralized\u2014meaning outside their control\u2014for years.
— Edward Snowden (@Snowden) December 30, 2017
More from Category c19


It's all here folks...How the CoVid Con was 37 years in the marking
3/4
https://t.co/WBAnAUO0UU
3/4
https://t.co/WBAnAUO0UU
Finally, this film demonstrates that EVERY SINGLE aspect of the fraudulent "science" used to the sell SARS-2=CoVid fraud was perfected in the 1980s to sell the HIV=AIDS fraud. https://t.co/Gjqo2lGjQw
— Ken McCarthy (@KenMcCarthy) March 10, 2021



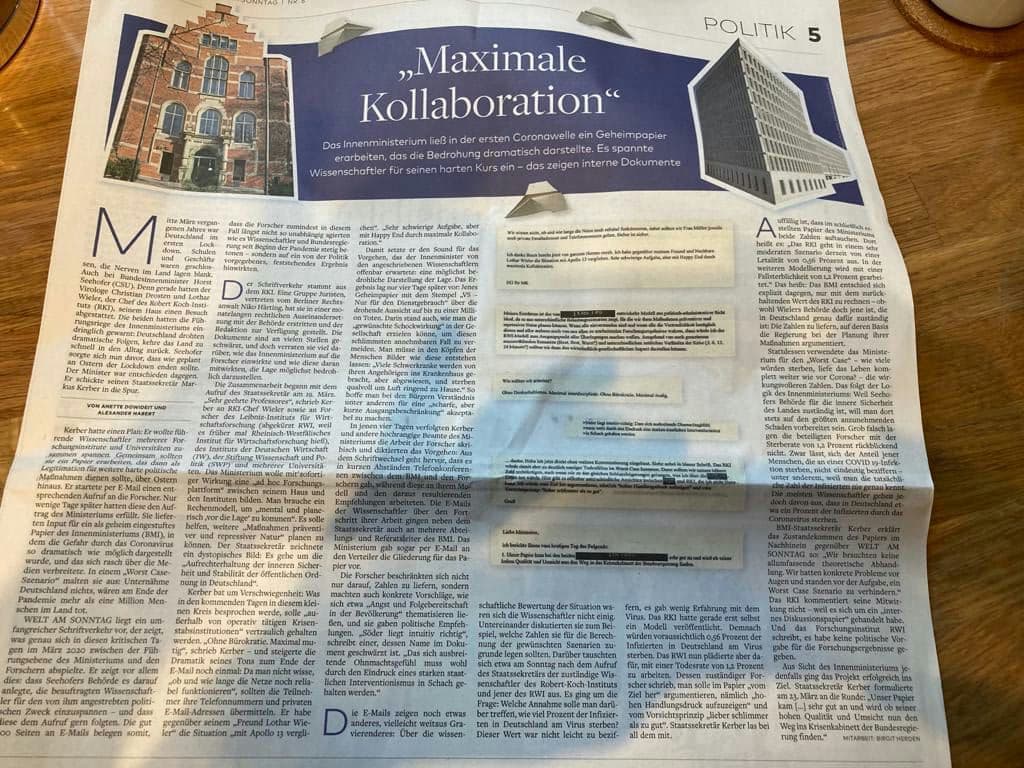
@welt published an article today on the “panic paper”-scandal in Germany.
Title is "Maximum collaboration”, showing @BMI_Bund / Horst Seehofer had a secret paper drafted in the 1st COVID-19 wave that dramatically depicted the threat.
A scandal of gigantic proportions. Thread⬇️
2/: @welt released 2 versions: long version as print, short-edit, online.
This thread focuses on the long version. It's of crucial importance-people around the globe understand this earthshaking scandal. Share.
English: https://t.co/qAbU6D8c0P
German: https://t.co/W2i1FtVrCg
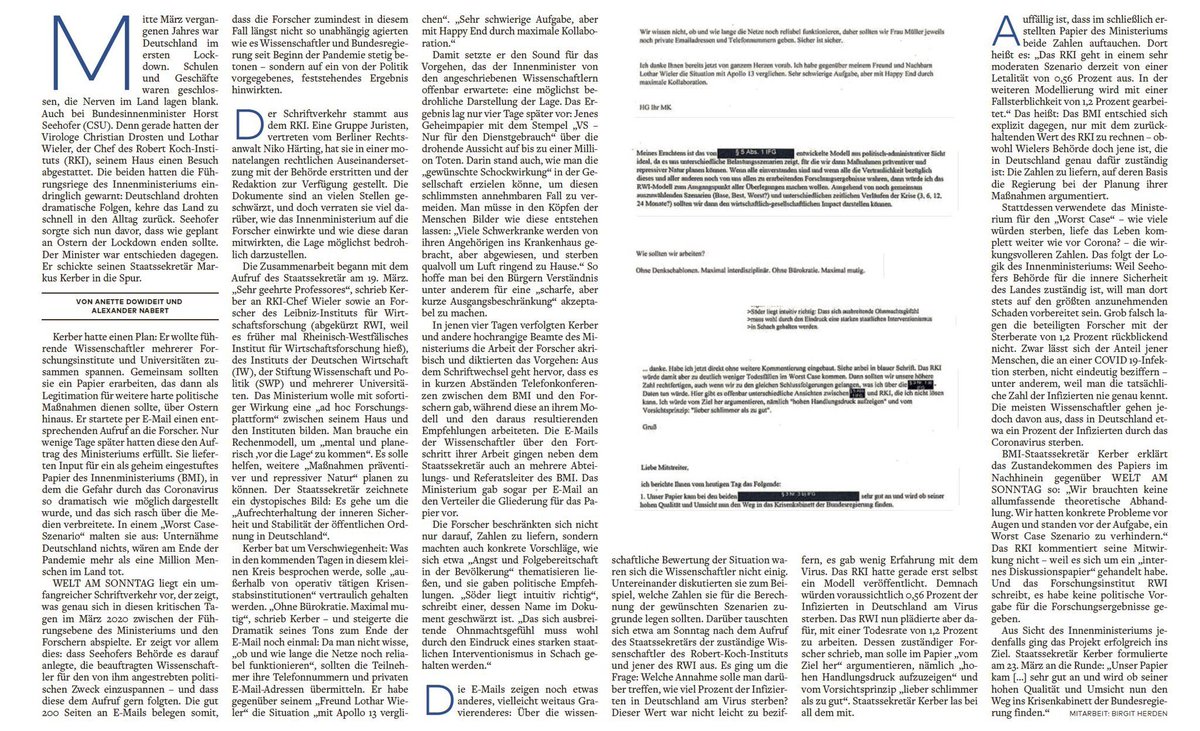
3/: Mid-March 2020: Federal Minister of the Interior-Horst Seehofer (@BMI_Bund, @cducsubt) was on the edge: Christian Drosten (@c_drosten) & Lothar Wieler (@RKI) urgently warned: Germany was threatened w/ dramatic consequences if the country returned to everyday life too quickly.

4/: Horst Seehofer sent his Secretary of State Markus Kerber into the lane. The plan was to bring together leading scientists: they should produce a paper that would then serve as legitimation for further tough political measures, beyond Easter - now known as the “panic paper”.
5/: Markus Kerber launched a corresponding call to researchers via e-mail, 4 days later, the request was fulfilled: A classified paper, which presented the danger posed by the virus as dramatically as possible, and which quickly spread through the media.

Title is "Maximum collaboration”, showing @BMI_Bund / Horst Seehofer had a secret paper drafted in the 1st COVID-19 wave that dramatically depicted the threat.
A scandal of gigantic proportions. Thread⬇️
2/: @welt released 2 versions: long version as print, short-edit, online.
This thread focuses on the long version. It's of crucial importance-people around the globe understand this earthshaking scandal. Share.
English: https://t.co/qAbU6D8c0P
German: https://t.co/W2i1FtVrCg
3/: Mid-March 2020: Federal Minister of the Interior-Horst Seehofer (@BMI_Bund, @cducsubt) was on the edge: Christian Drosten (@c_drosten) & Lothar Wieler (@RKI) urgently warned: Germany was threatened w/ dramatic consequences if the country returned to everyday life too quickly.
4/: Horst Seehofer sent his Secretary of State Markus Kerber into the lane. The plan was to bring together leading scientists: they should produce a paper that would then serve as legitimation for further tough political measures, beyond Easter - now known as the “panic paper”.
5/: Markus Kerber launched a corresponding call to researchers via e-mail, 4 days later, the request was fulfilled: A classified paper, which presented the danger posed by the virus as dramatically as possible, and which quickly spread through the media.