
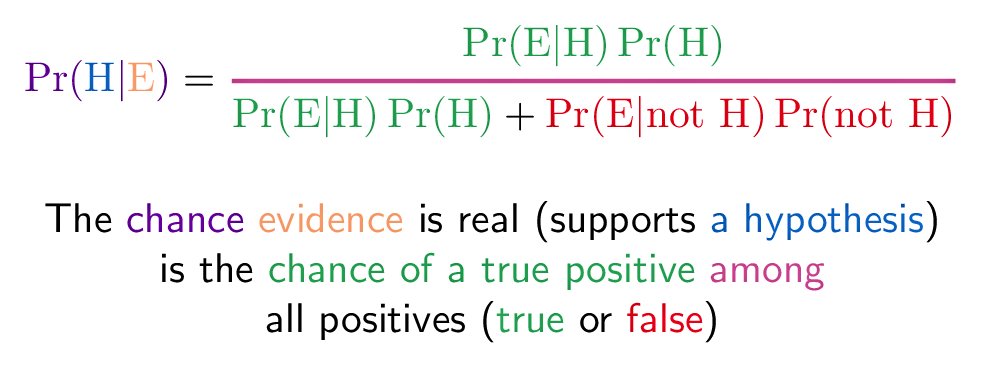
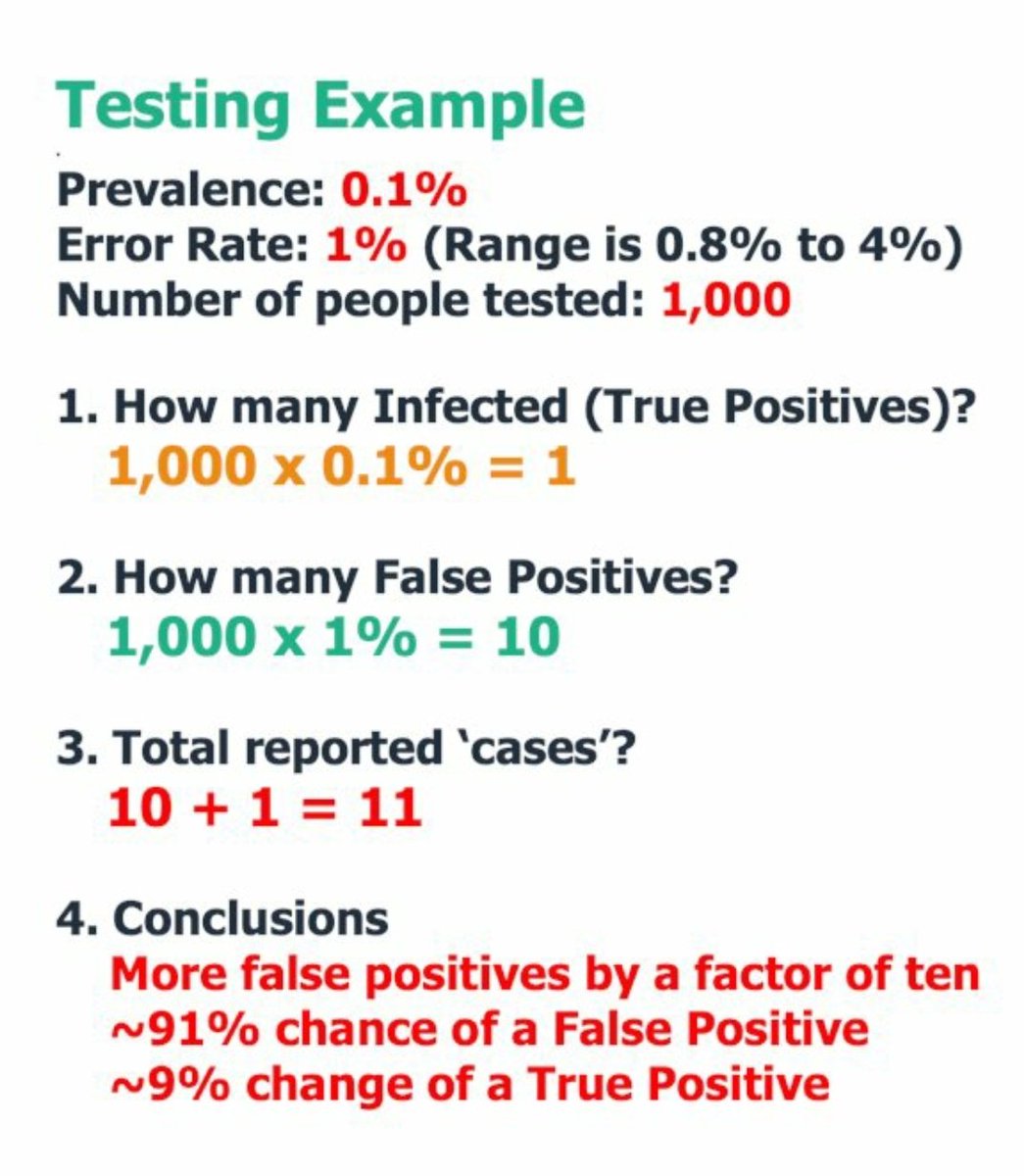
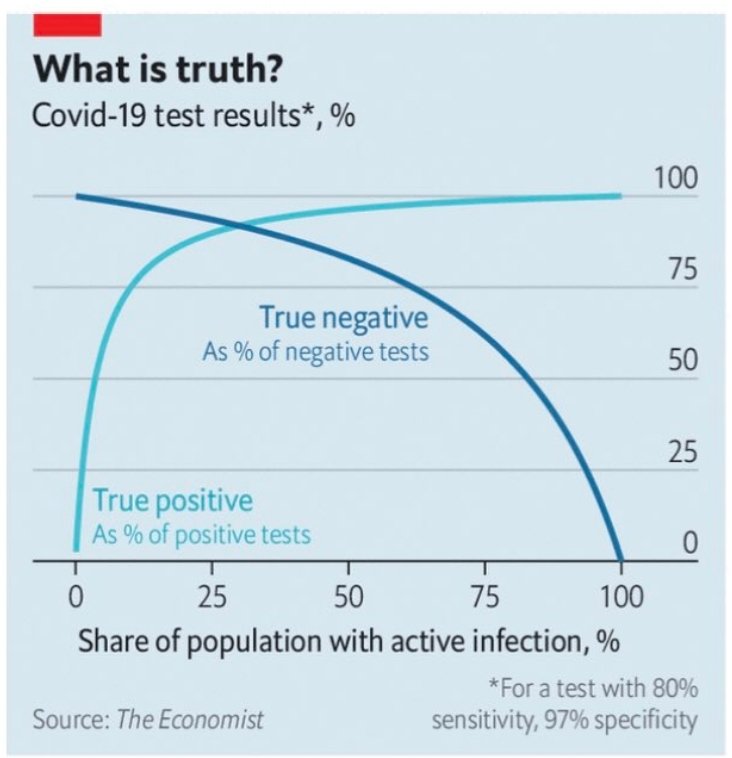
BAYES' THEOREM: The basic reason we get so many false positives to COVID19. The disease is so rare that the number of false positives greatly outnumbers the people who truly have the disease: THE MATHS:
https://t.co/oLHyxYJW9H

https://t.co/29FNwq0Qw2
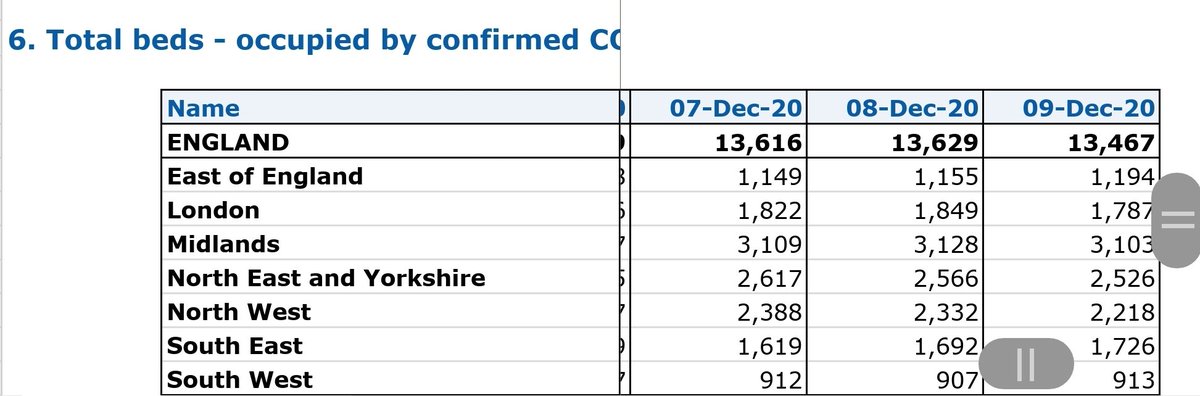
"The national statistician has downgraded its estimate of coronavirus in England on October 17 to just 4.89 people per 10,000." or ~ 0.05%. That means that only 1 in 2000 people may be carrying SARS related viral RNA fragments which could be 2 months old. https://t.co/XqpNaY6BzQ
— Robin Monotti FRSA MA BSc (@robinmonotti) December 8, 2020
https://t.co/rthjPRJWeB
ITALY: CONFIRMED BY ITALIAN HEALTH SERVICE: False positives to Covid19 test as diagnosis are 95%. Legal cases started against testing under charges of fraud to procure public funding, false alarm, ideological false, and manslaughter. pic.twitter.com/C9b7BbzdKa
— Robin Monotti FRSA MA BSc (@robinmonotti) November 25, 2020
#BAYESTHEOREM MEDICAL MASS TESTING CALCULATOR:
— Robin Monotti FRSA MA BSc (@robinmonotti) December 9, 2020
Try it yourself to understand how many false positives you get by changing minor variables: \U0001f447https://t.co/7wVMvrpgAW pic.twitter.com/PHbweWK1TK
https://t.co/kFnQVoCspb
LATERAL FLOW: False positive rate of "0.4% with a sensitivity of 58% and specificity of 99.6%, would mean that 100\u2009000 people being tested would find 630 positives\u2014of which only 230 would actually have covid-19, while 400 would be false positives.
— Robin Monotti FRSA MA BSc (@robinmonotti) November 17, 2020
https://t.co/8hsZ1hNjD7
Official estimates from mass testing in England (including asymptomatic) puts Covid19 "infections" at 0.9% https://t.co/2ljzi9YfKN
— Robin Monotti FRSA MA BSc (@robinmonotti) December 11, 2020
@lucyfrazermp 20/11:
— Edmund Fordham (@EdmundFordham) November 28, 2020
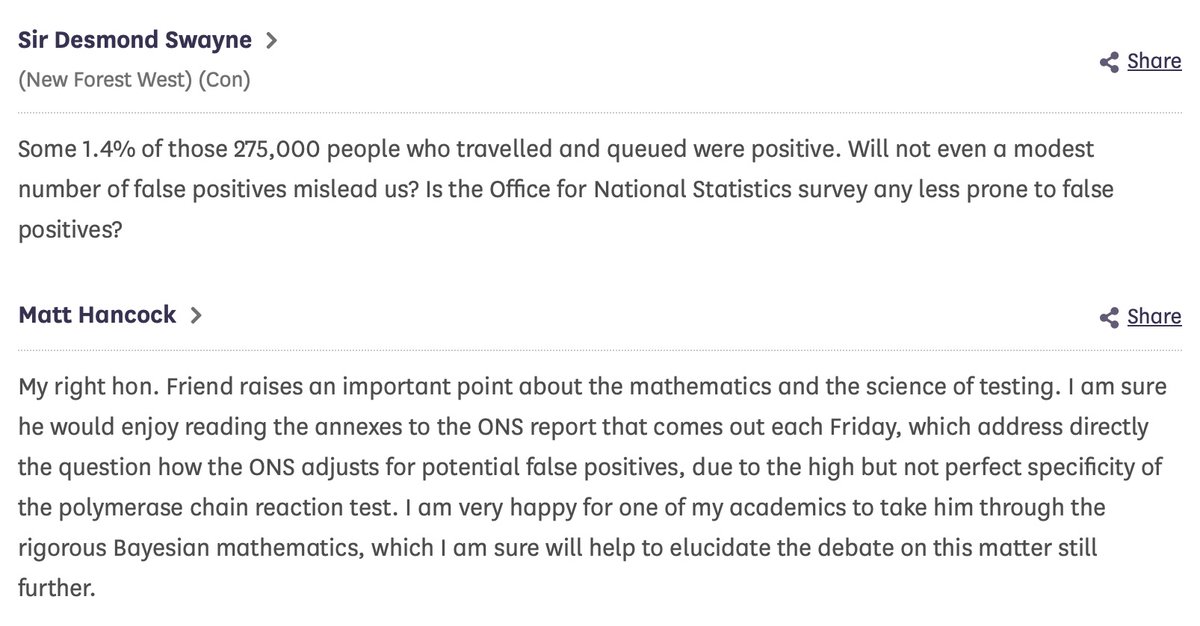
2. Apparently @MattHancock tells HoC 17/09 how ONS \u201cadjusts for False Positives\u201d. Looked it up.@DesmondSwayne asks;@MattHancock doesn\u2019t answer.
Obfuscates with \u201crigorous Bayesian mathematics\u201d
\u201cOne of his academics" will \u201ctake him through it\u201d
(thread) pic.twitter.com/42YO9vaioy
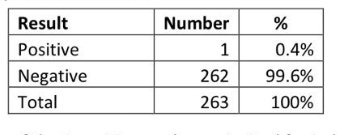
#BAYESTHEOREM @ Cambridge University. 0.4% of 262 students came back as positive after the first "test". All came back as negative after the second. Government only tests once. ONS would say there is 0.4% prevalence instead it's 0%. pic.twitter.com/zeAQAAOeRN
— Robin Monotti FRSA MA BSc (@robinmonotti) December 13, 2020
https://t.co/pZcFlMBKEZ
"I am very happy for one of my academics to take him through the rigorous Bayesian mathematics, which I am sure will help to elucidate the debate on this matter still further." @MattHancock to @DesmondSwaynehttps://t.co/pZcFlMBKEZ
— Robin Monotti FRSA MA BSc (@robinmonotti) December 15, 2020
https://t.co/aidVGWOVqH
Numerical details aside, the use of Bayes's theorem and the principle described are valid. Taught in epidemiology courses.
— \u05e4\u05e8\u05d5\u05e4' \u05d0\u05d9\u05d9\u05dc \u05e9\u05d7\u05e8 (@prof_shahar) December 16, 2020
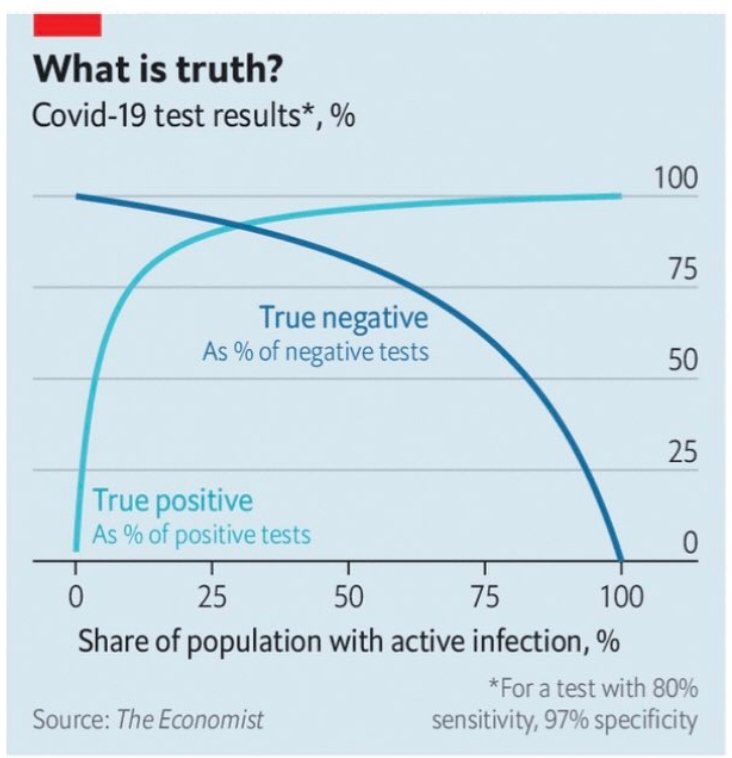
Extreme example. If disease prevalence is zero, predictive value of positive test is zero. Every positive is false positive.
A similar graph in the thread pic.twitter.com/ddvBe36OmU
\u26a0\ufe0fWHO WARNING ON BAYES THEOREM & TESTING \u26a0\ufe0f
— Robin Monotti FRSA MA BSc (@robinmonotti) December 16, 2020
"Healthcare providers are encouraged to take into consideration testing results along with clinical signs and symptoms, confirmed status of any contacts"https://t.co/GkRJzdn70b pic.twitter.com/jXPQDqqnVE
More from Robin Monotti FRSA MA BSc
Italian researchers: vaccines will not work against SARSCoV2 because this virus does not only replicate in human cells like other viruses, this one replicates through bacteria too. This is the fundamental reason why antibiotics work & vaccines will not:
Here is the Italian-EU scientific study indicating SARSCoV2 replicates in bacteria, not only human cells, and that is why antibiotics work and these vaccines will not:
"The preliminary results suggest that SARS-CoV-2 replicates in bacterial
2 of the 4 authors of the study work at the European Commission. Another works at an Italian medical research facility called Craniomed: https://t.co/EETSM3nb3T
You can find all of CRANIOMED's Carlo Brogna's published scientific research articles here, take a look:
Here is the Italian-EU scientific study indicating SARSCoV2 replicates in bacteria, not only human cells, and that is why antibiotics work and these vaccines will not:
"The preliminary results suggest that SARS-CoV-2 replicates in bacterial
2 of the 4 authors of the study work at the European Commission. Another works at an Italian medical research facility called Craniomed: https://t.co/EETSM3nb3T
You can find all of CRANIOMED's Carlo Brogna's published scientific research articles here, take a look:
More from Category c19

1/: The Nuremberg Code is a set of research ethics principles for human experimentation created as a result of the Nuremberg trials at the end of the Second World War. In light of the current events, they are more actual than ever before. ⬇️an important thread⬇️
2/: These so-called ‘Doctors’ Trial’ focused on physicians who conducted #inhumane and #unethical human experiments in German concentration camps, in addition to those who were involved in over 3,500,000 sterilizations of German citizens. (the picture shows doctors/criminals)

3/: Ten points of the code were given in the section of the verdict entitled "Permissible Medical Experiments". They can be found in detail on the following website:
4/: Point #1 means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, or deceit.
5/: Using an insufficiently-tested vaccine on humans is unethical. However, as long as people voluntarily consent to receive the vaccine, being informed about all risks, everything is OK. Doing this with force, however, is against the Nuremberg Code.
2/: These so-called ‘Doctors’ Trial’ focused on physicians who conducted #inhumane and #unethical human experiments in German concentration camps, in addition to those who were involved in over 3,500,000 sterilizations of German citizens. (the picture shows doctors/criminals)
3/: Ten points of the code were given in the section of the verdict entitled "Permissible Medical Experiments". They can be found in detail on the following website:
4/: Point #1 means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, or deceit.
5/: Using an insufficiently-tested vaccine on humans is unethical. However, as long as people voluntarily consent to receive the vaccine, being informed about all risks, everything is OK. Doing this with force, however, is against the Nuremberg Code.
Important - share: Camera footage out of care homes (USA, corrected), provided by @RobertKennedyJr's team. You can clearly see: Collateral Damages, Army assisting, force, death.
— Bobby Rajesh Malhotra \u30c4 (@Bobby_Network) February 17, 2021
Worldwide phenomen, also in Germany:https://t.co/GV7gqiPl1u
21st Century Nuremberg Trials-material pic.twitter.com/wPekgPYHIR

1/12
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
4/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
...indication, first of all that testing for a (single) respiratory virus is done outside of surveillance systems or need for specific therapy, but even so the lack of consideration of Ct, symptoms and clinical findings when interpreting its result. https://t.co/gHH6kwRdZG
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
6/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
The neither validated nor standardised hypersensitive RT-PCR test / Ct 35-45 for SARS-CoV-2 is abused to mislabel (also) other diseases, especially influenza, as COVID-19.https://t.co/AkFIfTCTkS
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.https://t.co/mbNY8bdw1p pic.twitter.com/OQBD4grMth
— Dr. Thomas Binder, MD (@Thomas_Binder) November 29, 2020
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
Thread web\u2b06\ufe0f\u2b07\ufe0f
— Dr. Thomas Binder, MD (@Thomas_Binder) December 16, 2020
The fabrication of the "asymptomatic (super) spreader" is the coronation of the total nons(ci)ense in the belief system of #CoronasWitnesses.
Asymptomatic transmission 0.7%; 95% CI 0%-4.9% - could well be 0%!https://t.co/VeZTzxXfvT
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
8/8
— Dr. Thomas Binder, MD (@Thomas_Binder) March 24, 2020
By the way, who the f*** created this obviously (almost) worldwide definition of #CoronaDeath?
This is not only medical malpractice, this is utterly insane!https://t.co/FFsTx4L2mw



Let's talk about MASKS!

Thread 1:
Masks increase mortality because breathing through them nebulizes aerosols into smaller ones which bypass mucosal immunity & reach all the way into the alveoli, leading to acute respiratory distress syndrome (ARDS).
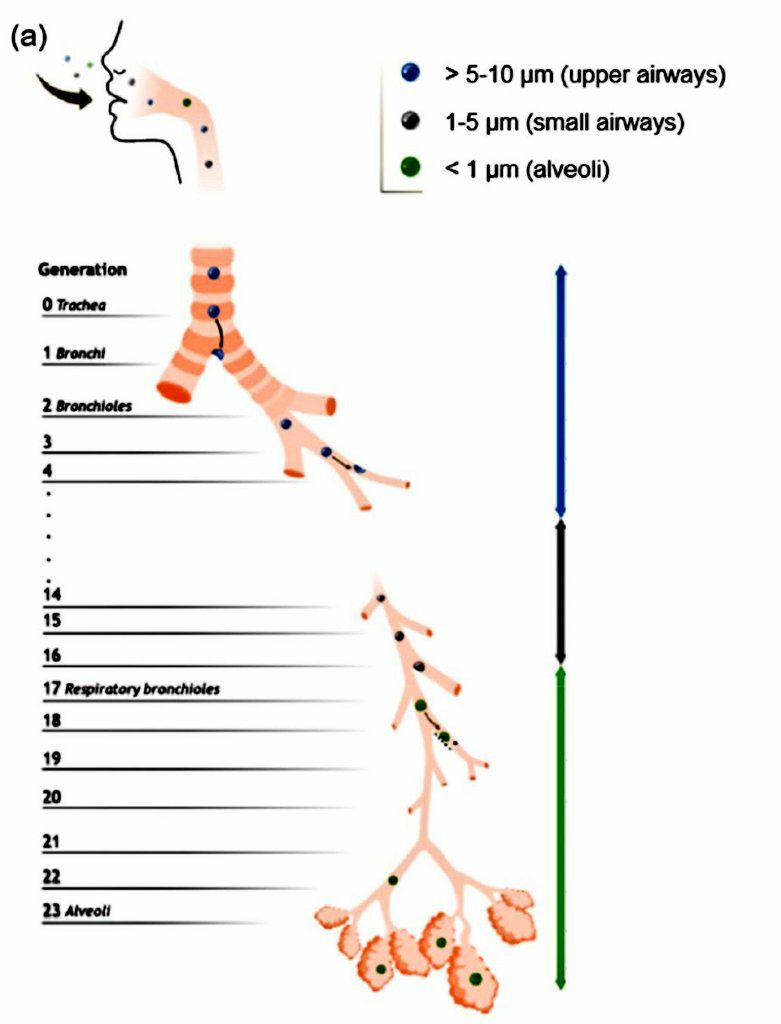
"Aerosols..within the most breathable size range between 0.5 & 5 μm, can carry SARS-CoV-2 deep to the terminal alveoli..if this transmission pathway does exist, it would bypass the mucociliary clearance & incubation period of the virus in the upper
The filtration material itself of N95's average pore size ~0.3−0.5 μm does not block finer aerosol laden with virions penetration, not to mention surgical masks.
Thread 1:
If you study the field you will see viral nebulization is a technique used to get higher infectivity of viruses. This is used with ventilator patients suffering from pseudomonas aeruginosa infections. Nebulize bacteriaphage to get deep into the lungs and kill bacteria. pic.twitter.com/82lNRMrXl4
— Kevin McKernan \U0001f642 (@Kevin_McKernan) October 24, 2020
Masks increase mortality because breathing through them nebulizes aerosols into smaller ones which bypass mucosal immunity & reach all the way into the alveoli, leading to acute respiratory distress syndrome (ARDS).
"Aerosols..within the most breathable size range between 0.5 & 5 μm, can carry SARS-CoV-2 deep to the terminal alveoli..if this transmission pathway does exist, it would bypass the mucociliary clearance & incubation period of the virus in the upper
The filtration material itself of N95's average pore size ~0.3−0.5 μm does not block finer aerosol laden with virions penetration, not to mention surgical masks.




















