
LIST OF QUESTIONS FOR MPS
From @ClareCraigPath and Dr Jonathan Engler:
.
1.Why are SARS-CoV-2 antibody levels flat or dropping across all age groups since May if the pandemic is still going?
https://t.co/SAVtoyNbia
#COVID19 letter to #MPs
— Ian James Seale (@IanJamesSeale) November 28, 2020
Pleas Copy/Paste, e-mail and RT.
Drs' Claire Craig FRCPath & Jonathan Engler, have kindly written the following list of 20 questions, which demand answers, especially prior to any vote regarding SARS-Cov-2, Covid-19 restrictions.https://t.co/nj1GIlEUOw
More from Robin Monotti Graziadei

I’m not just a lockdown sceptic. I know lockdowns increase infections rather than decrease them because I read research first hand. I’m a citizen in a democracy who wants Government policy to be evidence-based, not epidemiological modelling based. Crazy, I know.
Lockdowns increase infections because they lower immunity & therefore increase the disease. After hospitals & care homes households account for the largest number of transmissions. Schools/universities act as a break in transmission of the disease. All evidence based.
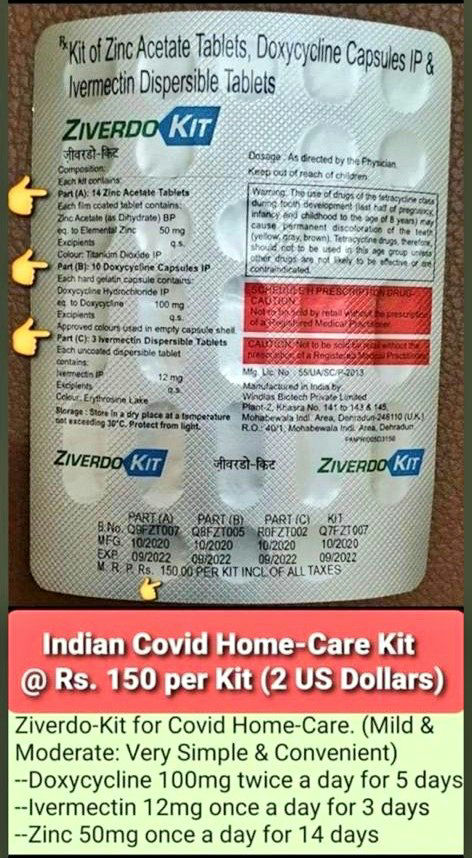
Transmission does not mean infection. I can transmit SARSCoV2 but I can't transmit Covid19. Whether SARSCoV2 develops at all into mild or severe Covid19 depends entirely on the immune system of the recipient. Early treatment prevents severe Covid19, the right treatment cures it.
"Children act more as a brake on infection," said Prof. Reinhard Berner, the head of pediatric medicine at Dresden University Hospital and leader of the study. "Not every infection that reaches them is passed
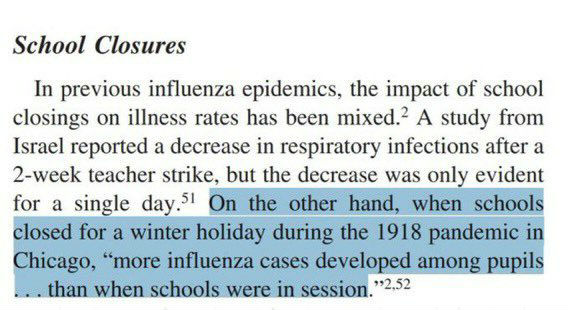
Closing schools increases transmission of respiratory viral infection because children act as a break on the community transmission of the virus. We have known this since 1918:
https://t.co/TPRYQ1LAAJ
Lockdowns increase infections because they lower immunity & therefore increase the disease. After hospitals & care homes households account for the largest number of transmissions. Schools/universities act as a break in transmission of the disease. All evidence based.
Transmission does not mean infection. I can transmit SARSCoV2 but I can't transmit Covid19. Whether SARSCoV2 develops at all into mild or severe Covid19 depends entirely on the immune system of the recipient. Early treatment prevents severe Covid19, the right treatment cures it.
"Children act more as a brake on infection," said Prof. Reinhard Berner, the head of pediatric medicine at Dresden University Hospital and leader of the study. "Not every infection that reaches them is passed
Closing schools increases transmission of respiratory viral infection because children act as a break on the community transmission of the virus. We have known this since 1918:
https://t.co/TPRYQ1LAAJ
More from Education






I get asked a lot how you can improve your skills and chances of getting a job as a developer. Best way is to work on a real-world project, deploy it, make it open-source, get feedback from others, share your knowledge, rinse, repeat.
Here are my top 7 project ideas. Thread 👇
1. 📊 Build an embeddable user feedback form (clone of https://t.co/xFHvT7iFEf) . Have a top notch design, fully working, minimal bugs, open-source, deploy it free on Heroku / Netlify / Vercel. If you can spare $11, buy a domain. Share with the whole world when done.
2. 🚀 Build a product roadmap SAAS.(https://t.co/Rq9DBeCMlh) Users can create new projects, create different stages for their projects. The community can submit project ideas, vote on existing ideas. Project owners pay a monthly fee per project.
3. ⛈️ Build a digital marketplace. (https://t.co/BWd1aeWMt5) Sellers can upload digital products for sale. Customers can purchase digital products and securely download. Sellers are paid out at the end of every month. Don't make it complicated, implement a great design.
4. 👨🏭 Build a job board software (https://t.co/EjWoMyqi9H). Companies can post jobs for a price, providing a link to the job application form. Jobs can be highlighted as urgent for an additional price.
Here are my top 7 project ideas. Thread 👇
1. 📊 Build an embeddable user feedback form (clone of https://t.co/xFHvT7iFEf) . Have a top notch design, fully working, minimal bugs, open-source, deploy it free on Heroku / Netlify / Vercel. If you can spare $11, buy a domain. Share with the whole world when done.
2. 🚀 Build a product roadmap SAAS.(https://t.co/Rq9DBeCMlh) Users can create new projects, create different stages for their projects. The community can submit project ideas, vote on existing ideas. Project owners pay a monthly fee per project.
3. ⛈️ Build a digital marketplace. (https://t.co/BWd1aeWMt5) Sellers can upload digital products for sale. Customers can purchase digital products and securely download. Sellers are paid out at the end of every month. Don't make it complicated, implement a great design.
4. 👨🏭 Build a job board software (https://t.co/EjWoMyqi9H). Companies can post jobs for a price, providing a link to the job application form. Jobs can be highlighted as urgent for an additional price.
You May Also Like






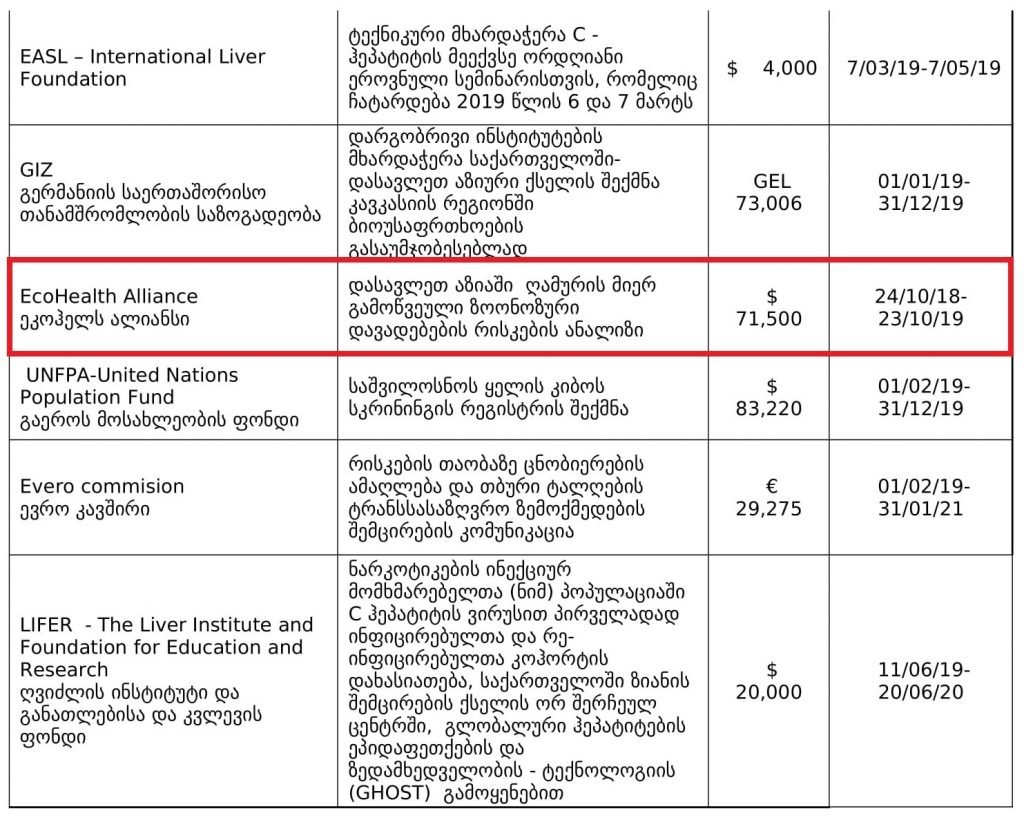
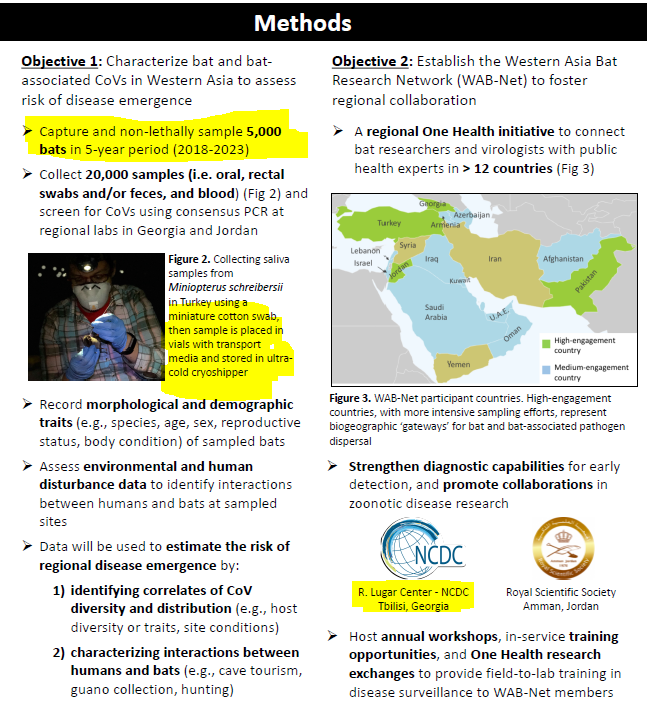
1. Project 1742 (EcoHealth/DTRA)
Risks of bat-borne zoonotic diseases in Western Asia
Duration: 24/10/2018-23 /10/2019
Funding: $71,500
@dgaytandzhieva
https://t.co/680CdD8uug
2. Bat Virus Database
Access to the database is limited only to those scientists participating in our ‘Bats and Coronaviruses’ project
Our intention is to eventually open up this database to the larger scientific community
https://t.co/mPn7b9HM48
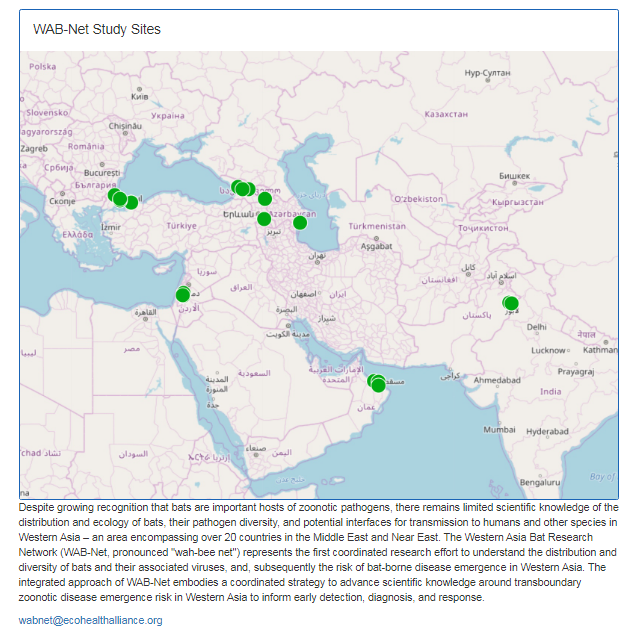
3. EcoHealth Alliance & DTRA Asking for Trouble
One Health research project focused on characterizing bat diversity, bat coronavirus diversity and the risk of bat-borne zoonotic disease emergence in the region.
https://t.co/u6aUeWBGEN
4. Phelps, Olival, Epstein, Karesh - EcoHealth/DTRA
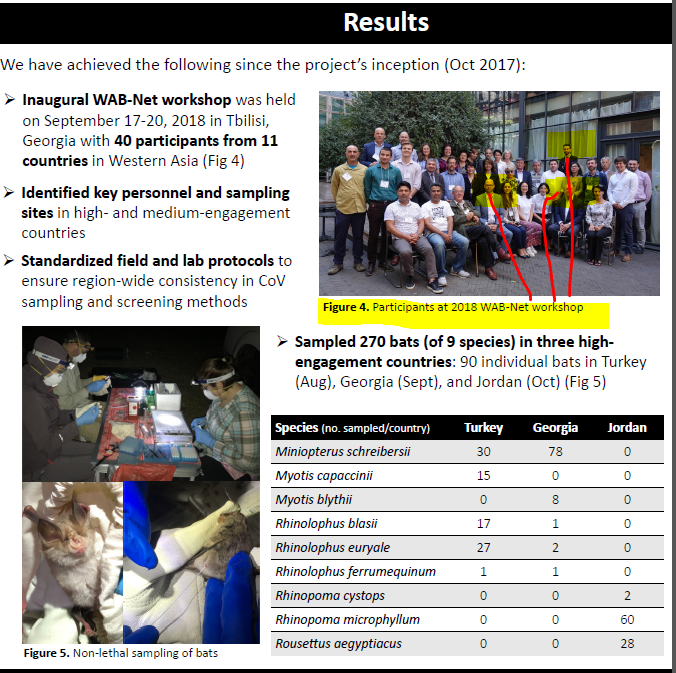
5, Methods and Expected Outcomes
(Unexpected Outcome = New Coronavirus Pandemic)
Risks of bat-borne zoonotic diseases in Western Asia
Duration: 24/10/2018-23 /10/2019
Funding: $71,500
@dgaytandzhieva
https://t.co/680CdD8uug
2. Bat Virus Database
Access to the database is limited only to those scientists participating in our ‘Bats and Coronaviruses’ project
Our intention is to eventually open up this database to the larger scientific community
https://t.co/mPn7b9HM48
3. EcoHealth Alliance & DTRA Asking for Trouble
One Health research project focused on characterizing bat diversity, bat coronavirus diversity and the risk of bat-borne zoonotic disease emergence in the region.
https://t.co/u6aUeWBGEN
4. Phelps, Olival, Epstein, Karesh - EcoHealth/DTRA
5, Methods and Expected Outcomes
(Unexpected Outcome = New Coronavirus Pandemic)
![Peter McCormack [Jan/3\u279e\u20bf \U0001f511\u220e]](https://pbs.twimg.com/profile_images/1524287442307723265/_59ITDbJ_normal.jpg)