Alex1Powell Categories Health




On the 19th March 2020 the WHO released this guidance intended for healthcare workers (HCWs), healthcare managers and IPC teams at the facility level & at national and district/provincial level:https://t.co/C4aV2BnMPj pic.twitter.com/tCk1EyLskV
— Robin Monotti (@robinmonotti) December 21, 2020
It clearly does indicate both the risks of bacterial infection & to prescribe broad spectrum antibiotics as part of treatment:
"Collect blood cultures for bacteria that cause pneumonia and sepsis, ideally before antimicrobial therapy. DO NOT
delay antimicrobial therapy"
"6. Management of severe COVID-19: treatment of co-infections
Give empiric antimicrobials [broad spectrum antibiotics] to treat all likely pathogens causing SARI and sepsis as soon as possible, within 1 hour
of initial assessment for patients with sepsis."
"Empiric antibiotic treatment should be based on the clinical diagnosis (community-acquired
pneumonia, health care-associated pneumonia [if infection was acquired in health care setting] or sepsis), local epidemiology &
susceptibility data, and national treatment guidelines"
"When there is ongoing local circulation of seasonal influenza, empiric therapy with a neuraminidase inhibitor [anti-viral influenza drugs] should
be considered for the treatment for patients with influenza or at risk for severe disease."

It’s just a big boost to insurer profits & will shutter independent physician practices & rural hospitals!
1/x
Just joined other House and Senate leaders in announcing a surprise billing agreement. Under this agreement, the days of patients receiving devastating surprise out-of-network medical bills will be over. https://t.co/HELY6OiPtS
— Rep. Frank Pallone (@FrankPallone) December 12, 2020
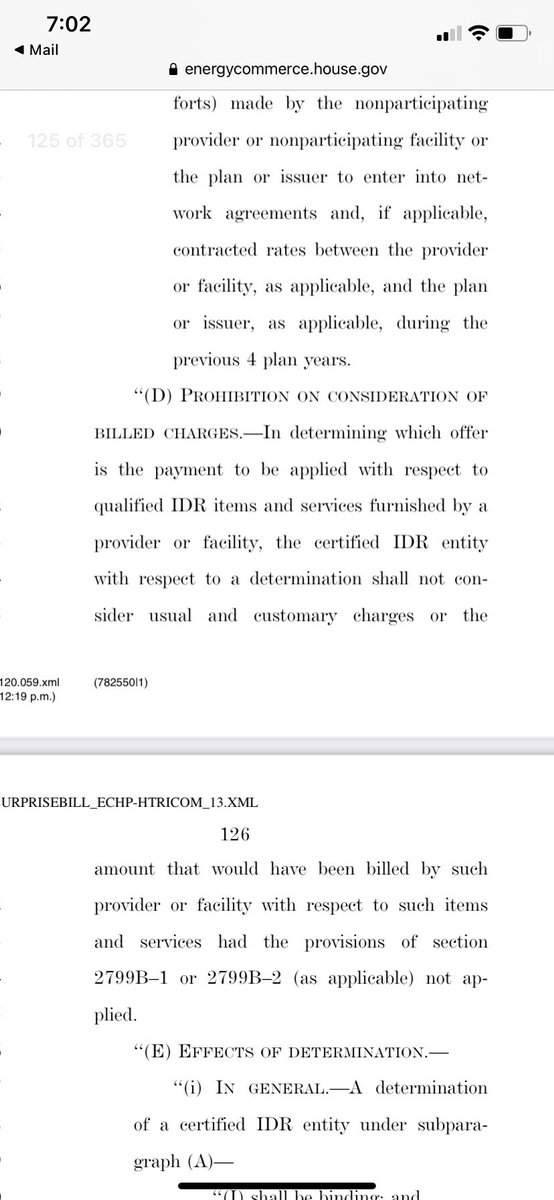
The Independent Dispute Resolution (IDR) in this compromise directs arbiter to consider “in network median rates” when settling disputes which is a sham arbitration & tantamount to benchmarking aka rate setting
Who dictates in network rates?
Insurers!
2/x
This bill prohibits use of charge data (aka usual & customary) which is another way of saying doctors must accept whatever poor contract terms or low balled payment offers insurers are jamming down their throats
This is just giving more power to profitable insurers
3/x
The reason why arbitration works in states like NY, TX is that it levels playing field, directs arbiters to consider independent price database like @FAIRHealth that can’t be manipulated by either side
Insurers have total control over “median in network” rates w their monopolies
When insurers have control over terms of arbitration, they will do everything in their power to do what any respectable publicly traded corporation will do: tilt the terms in their favor to increase





Because of the way I like teaching (research design, research methods and mechanics of research), ....
... I quickly realized that teaching Note-Taking Techniques, Reading Strategies, and Synthesis Methods was complicated. It's kind of a chicken and egg problem. What do students need to learn first, reading or taking notes? Teaching strategies for both is hard to do simultaneously
I tried the following sequence:
- Reading Strategies
- Note-Taking Techniques
- Synthesis Methods
- Writing Tips
Turns out that students are thrust into the "you need to read a lot to understand what I am teaching" model quite early during their programmes. This poses challenges
Normally, I would assign Adler and Van Doren's "How to Read a Book" https://t.co/F8vQIIKSfg so that my students can learn various levels of reading.
Only problem? A&VD is a massive 350 pages' book. Just imagine the amount of time it's going to take them to even *skim it*.
After teaching this class over the summer at ITAM and this fall at CIDE and FLACSO, at the Masters and PhD levels, and after decades of teaching undergraduates, I am convinced now that
(a) students need a range (repertoire) of reading strategies




It\u2019s disappointing that you would join an organization comprised of non-experts, spreading harmful misinformation about a pandemic.
— Alastair \u2018Wear a Mask\u2019 McAlpine (@AlastairMcA30) December 11, 2020
I would urge you to reconsider.
Here’s how @PanData19 is approaching this crisis differently from governments:
We believe that "health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity."- @WHO 2/n
To tackle the problem holistically, we have formed a multidisciplinary team made up of immunologist, microbiologist, geneticists, data scientists, physicians, economist, psychologists, educators, public health professionals and business owners. 3/n
We have also backed ourselves with a scientific advisory board made up of prominent experts in their fields.
@MartinKulldorff
@SunetraGupta
@MLevitt_NP2013
@MichaelYeadon3
#JayBhattacharya
#SucharitBhakdi
They are supporting us every step of the way. 4/n
We believe that "the right to health is one of a set of internationally agreed human rights standards, and is inseparable or ‘indivisible’ from these other rights.” @WHO 5/n













We assembled two mammalian expression vectors and one DNA cassette inserted into African Swine Fever from PRJNA607174! What happened in GuangDong at Mar-Aug 2019???!
The legitimacy of those “samples”—completely destroyed. The CoV-like sequences—cloned. No data from the pCoV group should ever be trusted in any way anymore!
Note: the DNA cassette exist in both unintegrated and integrated forms. Likely using homology-directed recombination. Whatever they were trying to express it is not just one or two proteins. There were also SV40 Ori which is yet to be properly mapped.
https://t.co/O1FYnwX6Oj
Why you need expression vectors in VERO since these cells are never used as expression hosts? Especially since there were a load of different tags on these vectors. The proteins had novel tags both N and C, IgK, His, Myc—especially His tag. This is for
NiNTA purification. There is no way that anyone would tag a protein this way and only use it to transfect VERO cells. There are no other host cells in these datasets other than Manis Javanica. Only Manis Javanica and Chlorocebus Aethiops. VERO is never used for recombinant

So let's take a look:
First up, some warning signs:
1) A generic username, and another real Twitter account (I've emailed)
2) No registration with GCRN
3) Only recently joined Twitter
On to the Issues.
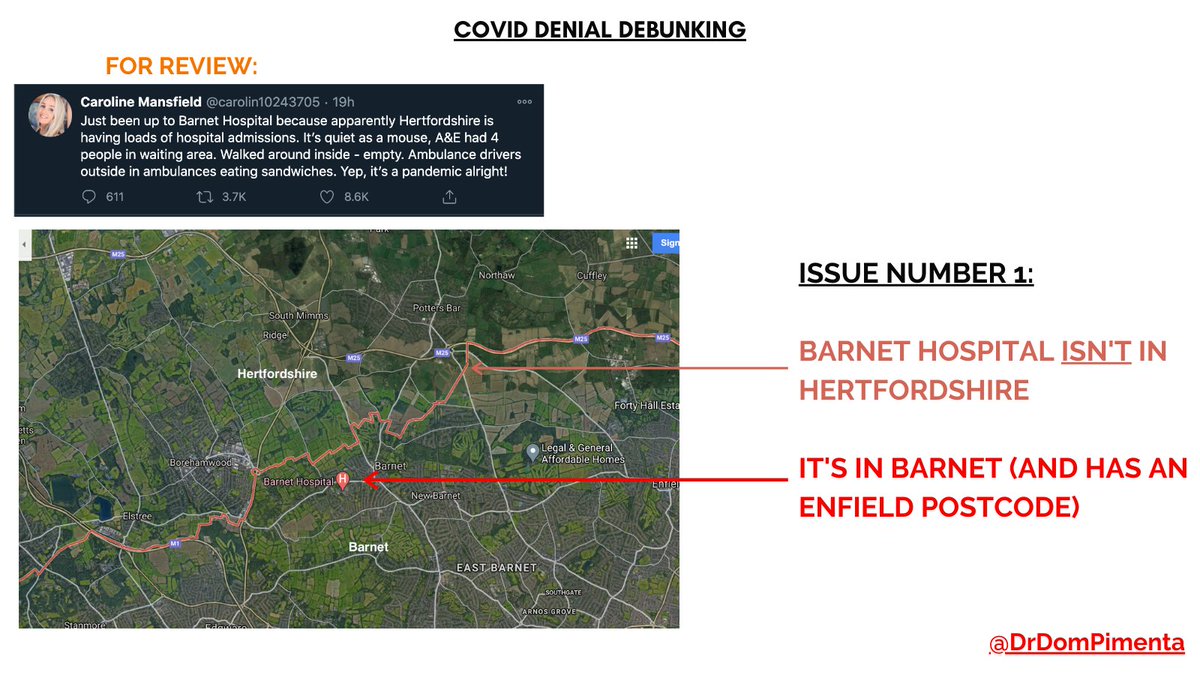
Issue No. 1: Barnet Hospital isn't actually IN Hertfordshire. It's in Barnet, with an Enfield postcode.
Which is confusing, but wouldn't be counted in Hertfordshire's hospital admission data.
Issue No. 2
Barnet is actually VERY busy with COVID cases, with 22% of our ENTIRE pandemic caseload in the LAST 7 DAYS ALONE
Source: https://t.co/IECfMo8FAK
Issue No. 3:
Barnet Hospital is seeing incredible pressures, the trust (The Royal Free Trust) has cancelled most non-urgent and routine work,
and as of 23rd Dec had admitted 244 patients with COVID, roughly half the peak of March, and climbing v. fast.
Issue No. 4
Even busier is Intensive Care - the whole trust only has 57 beds (23 - Barnet & 34 at the Royal Free Hospital).
As of 23rd Dec, 40 of them were occupied by COVID patients. That's 70% of the ENTIRE CAPACITY used up by COVID ALONE.
Source: https://t.co/zGmMSuoywN

If something "has teeth" it's effective
If it was "like pulling a tooth" it required effort to do.
Thus in comms it's used for plants working together and removal of dug-in plants.
e.g. S. Rich died July 2016
https://t.co/l9eUti2Wq9 symbolism signal
1. - Tooth Extracted Celebration Comms.
— CodesUcq (@CodesUcq) September 18, 2020
09/16/2020 Dentist Seth Lookhart extracted tooth July 2016 on hoverboard sentenced to 12 years
Note cheer after extraction in pic 3.
Does my expanding the article title give a clue as to the meaning? Yes it does.https://t.co/nOtO1DhnGy