
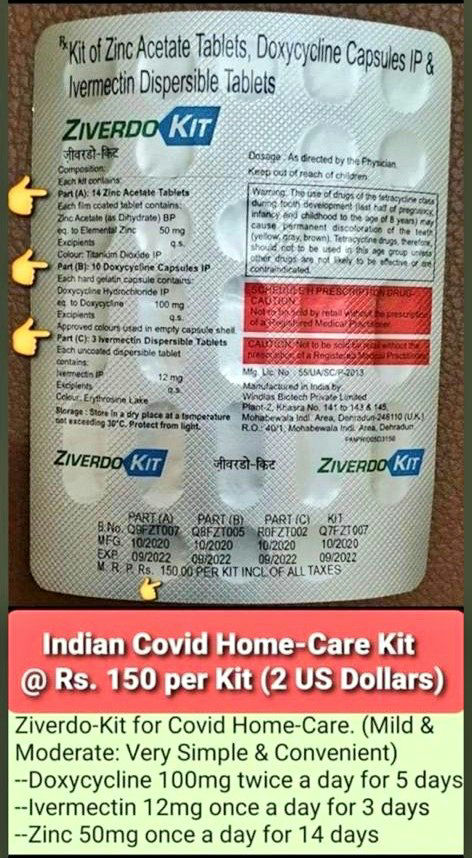
Can any MP ask the government why early treatment kits to stop viral replication & infection are not made available cheaply & prescription free in pharmacies as they are in India? Is it lives we want to save or is it Big Pharma profits? Because the two are mutually exclusive.
More from Robin Monotti
I’m not just a lockdown sceptic. I know lockdowns increase infections rather than decrease them because I read research first hand. I’m a citizen in a democracy who wants Government policy to be evidence-based, not epidemiological modelling based. Crazy, I know.
Lockdowns increase infections because they lower immunity & therefore increase the disease. After hospitals & care homes households account for the largest number of transmissions. Schools/universities act as a break in transmission of the disease. All evidence based.
Transmission does not mean infection. I can transmit SARSCoV2 but I can't transmit Covid19. Whether SARSCoV2 develops at all into mild or severe Covid19 depends entirely on the immune system of the recipient. Early treatment prevents severe Covid19, the right treatment cures it.
"Children act more as a brake on infection," said Prof. Reinhard Berner, the head of pediatric medicine at Dresden University Hospital and leader of the study. "Not every infection that reaches them is passed
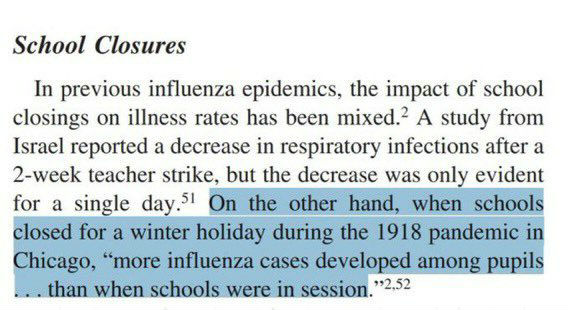
Closing schools increases transmission of respiratory viral infection because children act as a break on the community transmission of the virus. We have known this since 1918:
https://t.co/TPRYQ1LAAJ
Lockdowns increase infections because they lower immunity & therefore increase the disease. After hospitals & care homes households account for the largest number of transmissions. Schools/universities act as a break in transmission of the disease. All evidence based.
Transmission does not mean infection. I can transmit SARSCoV2 but I can't transmit Covid19. Whether SARSCoV2 develops at all into mild or severe Covid19 depends entirely on the immune system of the recipient. Early treatment prevents severe Covid19, the right treatment cures it.
"Children act more as a brake on infection," said Prof. Reinhard Berner, the head of pediatric medicine at Dresden University Hospital and leader of the study. "Not every infection that reaches them is passed
Closing schools increases transmission of respiratory viral infection because children act as a break on the community transmission of the virus. We have known this since 1918:
https://t.co/TPRYQ1LAAJ
The problem with meta-analysis like this is that it obfuscates the most important issue of treatment, which is timing.
This meta-analysis of controlled trials only looks at hospitalized patients. How long were the patients ill for before being hospitalized? One week? Two? Three? Too late for zinc ionophores (HCQ) (+ZINC? No zinc no point..) to work. Severe illness becomes bacterial in nature.
Was azythromycin administered when the bacterial infections were also too advanced? I have seen Azythromycin work with my very own eyes but that's not to say that if administered too late it may not save the patient. How many patients were given AZT & ventilated? It's all timing.
All the meta-analysis is telling us is if you leave it too late you may have missed the early window for antiviral zinc treatment (Zn+HCQ) & that if you are given AZT when you are ventilated or very severe it may too late for it to save you & corticosteroids may be last resort.
And of course antibiotics need also probiotics, or they may harm the bacterial flora which is part of the immune response. Difficult to tell from a meta-analysis how this problem was managed.
#BMJResearch update: Corticosteroids probably reduce mortality and mechanical ventilation in patients with covid-19 compared with standard care, whereas azithromycin, hydroxychloroquine, interferon-beta, and tocilizumab may not reduce either https://t.co/oQ3lTWUqaz
— The BMJ (@bmj_latest) December 18, 2020
This meta-analysis of controlled trials only looks at hospitalized patients. How long were the patients ill for before being hospitalized? One week? Two? Three? Too late for zinc ionophores (HCQ) (+ZINC? No zinc no point..) to work. Severe illness becomes bacterial in nature.
Was azythromycin administered when the bacterial infections were also too advanced? I have seen Azythromycin work with my very own eyes but that's not to say that if administered too late it may not save the patient. How many patients were given AZT & ventilated? It's all timing.
All the meta-analysis is telling us is if you leave it too late you may have missed the early window for antiviral zinc treatment (Zn+HCQ) & that if you are given AZT when you are ventilated or very severe it may too late for it to save you & corticosteroids may be last resort.
And of course antibiotics need also probiotics, or they may harm the bacterial flora which is part of the immune response. Difficult to tell from a meta-analysis how this problem was managed.
Twitter removed 800 followers from my account today. People have been writing saying twitter automatically unfollowed me for them. Follow me on Parler @robinmonotti & Telegram https://t.co/o5rFaSrCpa to bypass this.
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
Trust us not to turn over data. Trust us not to read your messages. Trust us not to close your channel. Maybe @Durov is an angel. I hope so! But angels have fallen before. Telegram should have been working to make channels decentralized\u2014meaning outside their control\u2014for years.
— Edward Snowden (@Snowden) December 30, 2017
More from Health








Thread on how atheism leads to mental retardation (backed with medical citations🧵💉)
To start with, atheism is an unnatural self-contradicting doctrine.
Medical terminology proves that human beings are naturally pre-disposed to believe in God. Oxford scientists assert that people are "born believers".
https://t.co/kE0Fi588yn
https://t.co/OqyXcGIMJn

It should be known that atheism could never produce an intelligently-functioning society and neither ever will.
Contrastingly, Islam produced several intellectuals & polymaths, was on the forefront of scientific development, boasting 100% literacy
It is also scientifically proven that atheism led to lesser scientific curiosity and scientific frauds, which is also why atheists incline to pseudo-science.
Whereas, religion in general and Islam in particular boosted education.
https://t.co/19Onc84u3g

Atheists are also likely to affected by pervasive mental and developmental disorders like high-functioning autism.
Cognitive Scientists and renowned Neurologists found that more atheism is leads to greater autism.
https://t.co/zRjEyFoX3P

To start with, atheism is an unnatural self-contradicting doctrine.
Medical terminology proves that human beings are naturally pre-disposed to believe in God. Oxford scientists assert that people are "born believers".
https://t.co/kE0Fi588yn
https://t.co/OqyXcGIMJn
It should be known that atheism could never produce an intelligently-functioning society and neither ever will.
Contrastingly, Islam produced several intellectuals & polymaths, was on the forefront of scientific development, boasting 100% literacy
If the Muslim world had not existed, there literally would be no technology/achievements today.
— Starks\u262a\ufe0f\U0001f1f9\U0001f1e9 (@MegaIntelIect) January 8, 2021
Science only developed because of Islam, Europe should be grateful to Islam for civilizing their barbaric cult.
Source: The Caliph's Splendor, Pg 204-05 https://t.co/HVypO52Tpc pic.twitter.com/00jYSbaDSs
It is also scientifically proven that atheism led to lesser scientific curiosity and scientific frauds, which is also why atheists incline to pseudo-science.
Whereas, religion in general and Islam in particular boosted education.
https://t.co/19Onc84u3g
Atheists are also likely to affected by pervasive mental and developmental disorders like high-functioning autism.
Cognitive Scientists and renowned Neurologists found that more atheism is leads to greater autism.
https://t.co/zRjEyFoX3P

You May Also Like



So the cryptocurrency industry has basically two products, one which is relatively benign and doesn't have product market fit, and one which is malignant and does. The industry has a weird superposition of understanding this fact and (strategically?) not understanding it.
The benign product is sovereign programmable money, which is historically a niche interest of folks with a relatively clustered set of beliefs about the state, the literary merit of Snow Crash, and the utility of gold to the modern economy.
This product has narrow appeal and, accordingly, is worth about as much as everything else on a 486 sitting in someone's basement is worth.
The other product is investment scams, which have approximately the best product market fit of anything produced by humans. In no age, in no country, in no city, at no level of sophistication do people consistently say "Actually I would prefer not to get money for nothing."
This product needs the exchanges like they need oxygen, because the value of it is directly tied to having payment rails to move real currency into the ecosystem and some jurisdictional and regulatory legerdemain to stay one step ahead of the banhammer.
If everyone was holding bitcoin on the old x86 in their parents basement, we would be finding a price bottom. The problem is the risk is all pooled at a few brokerages and a network of rotten exchanges with counter party risk that makes AIG circa 2008 look like a good credit.
— Greg Wester (@gwestr) November 25, 2018
The benign product is sovereign programmable money, which is historically a niche interest of folks with a relatively clustered set of beliefs about the state, the literary merit of Snow Crash, and the utility of gold to the modern economy.
This product has narrow appeal and, accordingly, is worth about as much as everything else on a 486 sitting in someone's basement is worth.
The other product is investment scams, which have approximately the best product market fit of anything produced by humans. In no age, in no country, in no city, at no level of sophistication do people consistently say "Actually I would prefer not to get money for nothing."
This product needs the exchanges like they need oxygen, because the value of it is directly tied to having payment rails to move real currency into the ecosystem and some jurisdictional and regulatory legerdemain to stay one step ahead of the banhammer.




