Seeing a lot of this circulating on the right, so let me explain why folks are worried even though it is not literally true that every ICU bed in the country is occupied at the moment.
it's disappointing to see that we are back in the "media scare stories about hospitals" stage.
— el gato malo (@boriquagato) December 7, 2020
the good news is that, just like last time, this is simply not the case.
they either have no idea what they are saying or are seeking to mislead.
let's look.https://t.co/eWyj2txAh6
1) Stretch existing workers to do more (potentially compromising care)
2) Recruit workers from other specialties (potentially compromising care)
2) Hire additional temporary workers
Of course, the patients also stay sick longer, which brings us to ...
That's very worrying because we might be 3 weeks from peak infections, & over a month from peak hospitalizations--falling as beds are still tied up w/Thanksgiving cases
An emergency too many people wish away by staring hard at isolated statistics & saying "I don't see a problem."
More from Health

You gotta think about this one carefully!
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
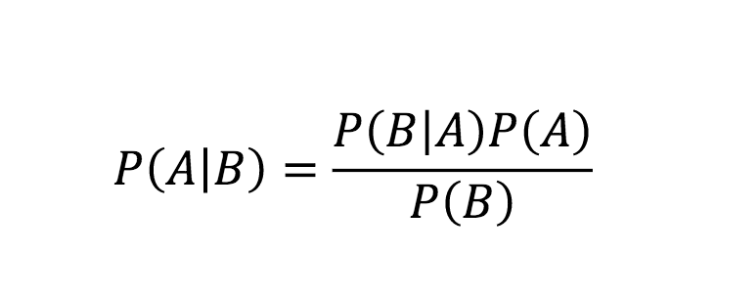
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
Really doesn\u2019t fit well in a tweet. pic.twitter.com/xN0pAyniFS
— Dr. Lena Sugar \U0001f3f3\ufe0f\u200d\U0001f308\U0001f1ea\U0001f1fa\U0001f1ef\U0001f1f5 (@_jvs) February 18, 2021
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇

No-regret #hydrogen:
Charting early steps for H₂ infrastructure in Europe.
👉Summary of conclusions of a new study by @AgoraEW @AFRY_global @Ma_Deutsch @gnievchenko (1/17)
https://t.co/YA50FA57Em
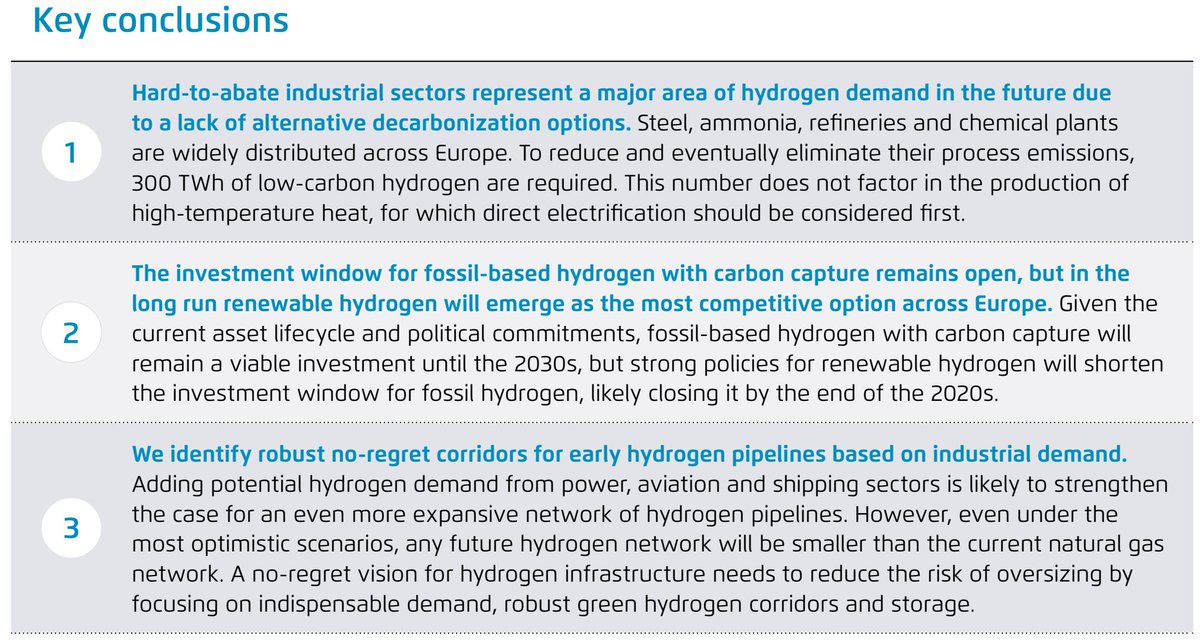
The idea behind this study is that future hydrogen demand is highly uncertain and we don’t want to spend tens of billions of euros to repurpose a network which won’t be needed. For instance, hydrogen in ground transport is a hotly debated topic https://t.co/RlnqDYVzpr (2/17)
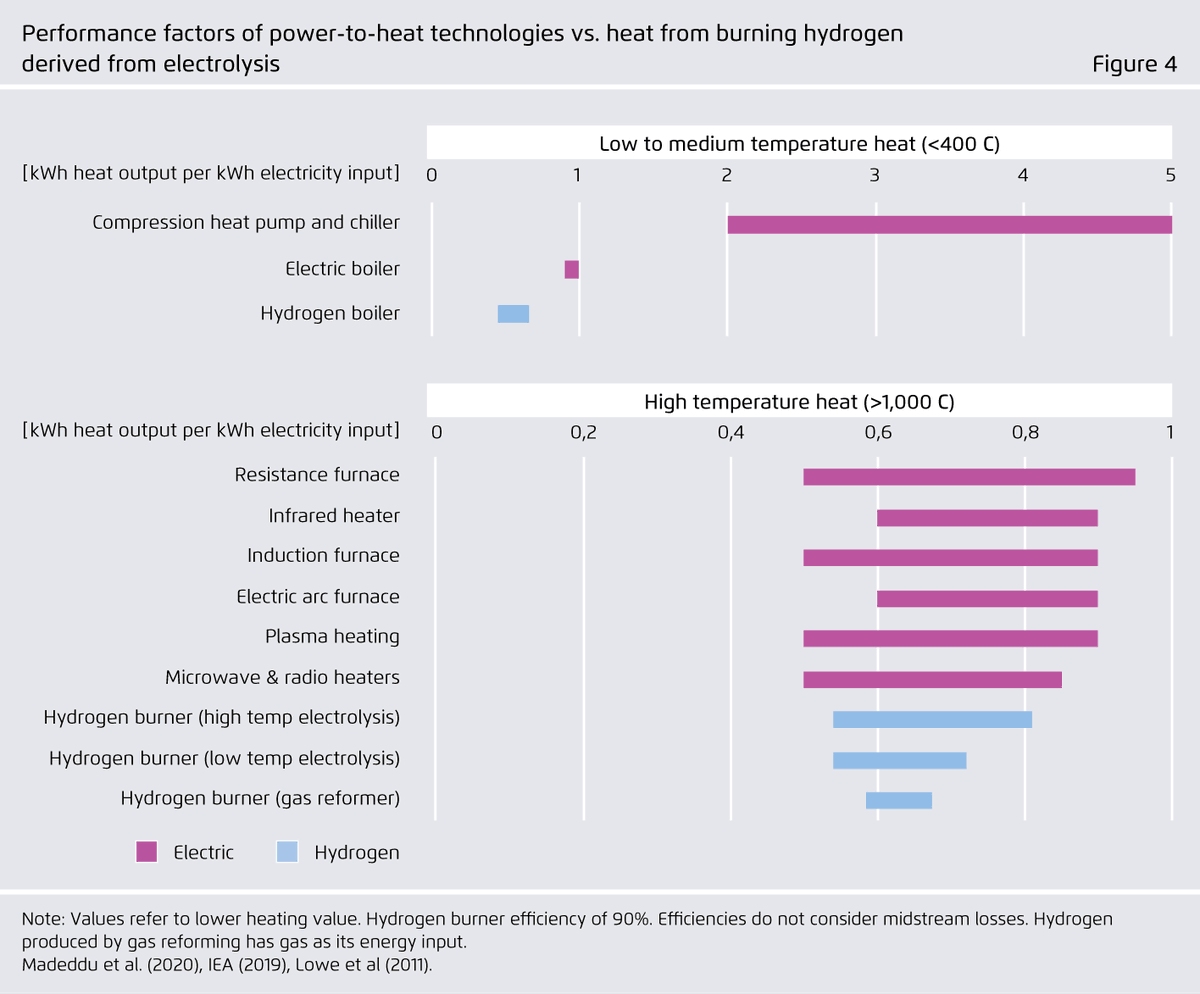
Similar things can be said about heat. 40% of today’s industrial natural gas use in the EU goes to heat below 100°C and therefore is within range of electric heat pumps – whose performance factors far exceed 100%. (3/17)

Even for higher temperatures, a range of power-to-heat (PtH) options can be more energy-efficient than hydrogen and should be considered first. Available PtH technologies can cover all temperature levels needed in industrial production (e.g. electric arc furnace: 3500°C). (4/17)
In our view, hydrogen use for feedstock and chemical reactions is the only inescapable source of industrial hydrogen demand in Europe that does not lend itself to electrification. Examples include ammonia, steel, and petrochemical industries. (5/17)
Charting early steps for H₂ infrastructure in Europe.
👉Summary of conclusions of a new study by @AgoraEW @AFRY_global @Ma_Deutsch @gnievchenko (1/17)
https://t.co/YA50FA57Em
The idea behind this study is that future hydrogen demand is highly uncertain and we don’t want to spend tens of billions of euros to repurpose a network which won’t be needed. For instance, hydrogen in ground transport is a hotly debated topic https://t.co/RlnqDYVzpr (2/17)
Similar things can be said about heat. 40% of today’s industrial natural gas use in the EU goes to heat below 100°C and therefore is within range of electric heat pumps – whose performance factors far exceed 100%. (3/17)
Even for higher temperatures, a range of power-to-heat (PtH) options can be more energy-efficient than hydrogen and should be considered first. Available PtH technologies can cover all temperature levels needed in industrial production (e.g. electric arc furnace: 3500°C). (4/17)
In our view, hydrogen use for feedstock and chemical reactions is the only inescapable source of industrial hydrogen demand in Europe that does not lend itself to electrification. Examples include ammonia, steel, and petrochemical industries. (5/17)