Categories Health

















We assembled two mammalian expression vectors and one DNA cassette inserted into African Swine Fever from PRJNA607174! What happened in GuangDong at Mar-Aug 2019???!
The legitimacy of those “samples”—completely destroyed. The CoV-like sequences—cloned. No data from the pCoV group should ever be trusted in any way anymore!
Note: the DNA cassette exist in both unintegrated and integrated forms. Likely using homology-directed recombination. Whatever they were trying to express it is not just one or two proteins. There were also SV40 Ori which is yet to be properly mapped.
https://t.co/O1FYnwX6Oj
Why you need expression vectors in VERO since these cells are never used as expression hosts? Especially since there were a load of different tags on these vectors. The proteins had novel tags both N and C, IgK, His, Myc—especially His tag. This is for
NiNTA purification. There is no way that anyone would tag a protein this way and only use it to transfect VERO cells. There are no other host cells in these datasets other than Manis Javanica. Only Manis Javanica and Chlorocebus Aethiops. VERO is never used for recombinant

If something "has teeth" it's effective
If it was "like pulling a tooth" it required effort to do.
Thus in comms it's used for plants working together and removal of dug-in plants.
e.g. S. Rich died July 2016
https://t.co/l9eUti2Wq9 symbolism signal
1. - Tooth Extracted Celebration Comms.
— CodesUcq (@CodesUcq) September 18, 2020
09/16/2020 Dentist Seth Lookhart extracted tooth July 2016 on hoverboard sentenced to 12 years
Note cheer after extraction in pic 3.
Does my expanding the article title give a clue as to the meaning? Yes it does.https://t.co/nOtO1DhnGy


NEW: a common response to reports of hospitals struggling this winter is "it\u2019s no different to a bad flu season!"
— John Burn-Murdoch (@jburnmurdoch) January 7, 2021
I\u2019ve tracked down historical data on flu ICU admissions, including winter 2017-18, a record high.
Here\u2019s how England\u2019s Covid winter compares to a bad flu season \U0001f4f9 pic.twitter.com/tsExrDZM31
27/42 Some sceptics arguing covid-19 tests are inaccurate. PCR tests not 100% accurate but hospital inpatient testing accuracy much increased by frequency of testing (typically admission, days 3 & 6/7, then weekly). This means very low numbers of overall false positives.
28/42 Some sceptics argue that the published covid-19 positive inpatient numbers include both those admitted with covid-19 and those who acquired covid-19 in hospital. And that there are significant numbers of patients who have acquired covid-19 in hospital.
29/42 Covid-19 positive test data has always included anyone testing positive, irrespective of initial diagnosis. And the NHS has always acknowledged that hospital acquired (nosocomial) infection is a big issue. Hospitals are working incredibly hard to control it….
30/42 …The NHS regularly and completely transparently publishes nosocomial infection data, by hospital. But neither issue affects the degree of pressure that hospitals are under. Every inpatient, irrespective of initial diagnosis/infection source, occupies a hospital bed.

So let's take a look:
First up, some warning signs:
1) A generic username, and another real Twitter account (I've emailed)
2) No registration with GCRN
3) Only recently joined Twitter
On to the Issues.
Issue No. 1: Barnet Hospital isn't actually IN Hertfordshire. It's in Barnet, with an Enfield postcode.
Which is confusing, but wouldn't be counted in Hertfordshire's hospital admission data.
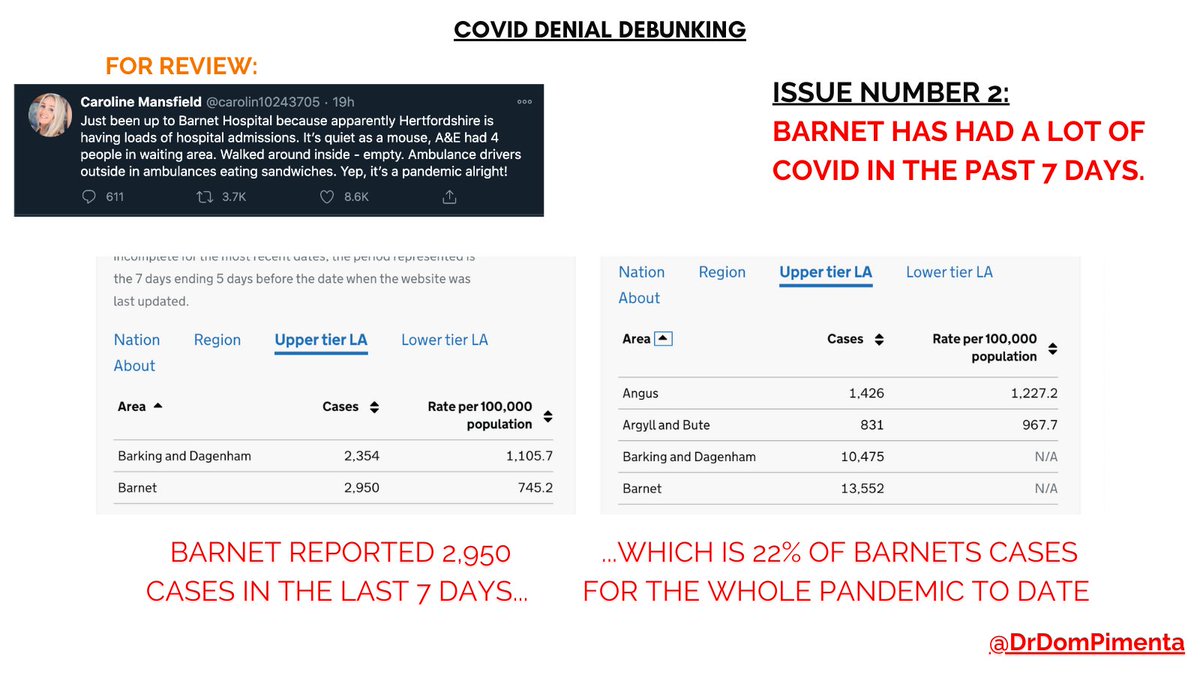
Issue No. 2
Barnet is actually VERY busy with COVID cases, with 22% of our ENTIRE pandemic caseload in the LAST 7 DAYS ALONE
Source: https://t.co/IECfMo8FAK
Issue No. 3:
Barnet Hospital is seeing incredible pressures, the trust (The Royal Free Trust) has cancelled most non-urgent and routine work,
and as of 23rd Dec had admitted 244 patients with COVID, roughly half the peak of March, and climbing v. fast.
Issue No. 4
Even busier is Intensive Care - the whole trust only has 57 beds (23 - Barnet & 34 at the Royal Free Hospital).
As of 23rd Dec, 40 of them were occupied by COVID patients. That's 70% of the ENTIRE CAPACITY used up by COVID ALONE.
Source: https://t.co/zGmMSuoywN




it's disappointing to see that we are back in the "media scare stories about hospitals" stage.
— el gato malo (@boriquagato) December 7, 2020
the good news is that, just like last time, this is simply not the case.
they either have no idea what they are saying or are seeking to mislead.
let's look.https://t.co/eWyj2txAh6
#1, the big worry is ICU space, not hospital beds, and as you can see from this very thread, ICU utilization is running well above hospital utilization generally.
#2 The constraint on ICUs isn't beds, it's staff. ICU beds are (relatively) easy to build. They're not much good if the only people you have to staff them are the cafeteria workers.
#3 It's true that ICUs can flex to deal with high utilization. But to do so, they have to:
1) Stretch existing workers to do more (potentially compromising care)
2) Recruit workers from other specialties (potentially compromising care)
2) Hire additional temporary workers
Hiring temps is the best strategy. The problem is, it's a good strategy that's hard to implement when a staggering fraction of the nation's hospitals are all having the same problems, requiring exactly the same skills from the same shrinking pool of workers, at the same time.

FIFTH Alaskan Experiences Anaphylaxis After Covid Vaccine - No Prior Allergies
Doctor Reports Serious Allergic Reaction to Moderna Vaccine https://t.co/Q5sNcczkTO
Oregon HCW -Severe Allergic Reaction https://t.co/BIQ6iEIVwT
Hamilton PSW Says Allergic Reaction to COVID-19 vaccine Led to Fainting, Seizures and CPR
Iowa Nurse Anaphylaxis Covid Vaccine https://t.co/WVKAsqdKzW
Mexican Doctor Hospitalized After Receiving Covid Vaccine (Encephalomyelitis)
Mexican Doctor In ICU: Transverse Myelitis After Covid Vaccine Mexican Doctor Hospitalized After Receiving Covid Vaccine (Encephalomyelitis) https://t.co/NOWVXYMGrh https://t.co/i1ezATTlbX
Massachusetts Nurse Anaphylaxis Covid Vaccine
Portuguese HCW, 41, Dies 2 Days After Covid Vaccine https://t.co/zjMKNw6IYu
Gregory Michael MD Death https://t.co/iJqYAIj2iU https://t.co/cHQDaWzh6y
HCW Karl Dunkin Severe Reaction to Covid Vaccine

