26/42 Are there any national datasets that accurately capture what is going on? The brilliant @jburnmurdoch has highlighted number of admissions into ICU. The message from his animated chart (click on link) couldn’t be clearer – this winter is v unusual: https://t.co/76ZvHU2pmV.
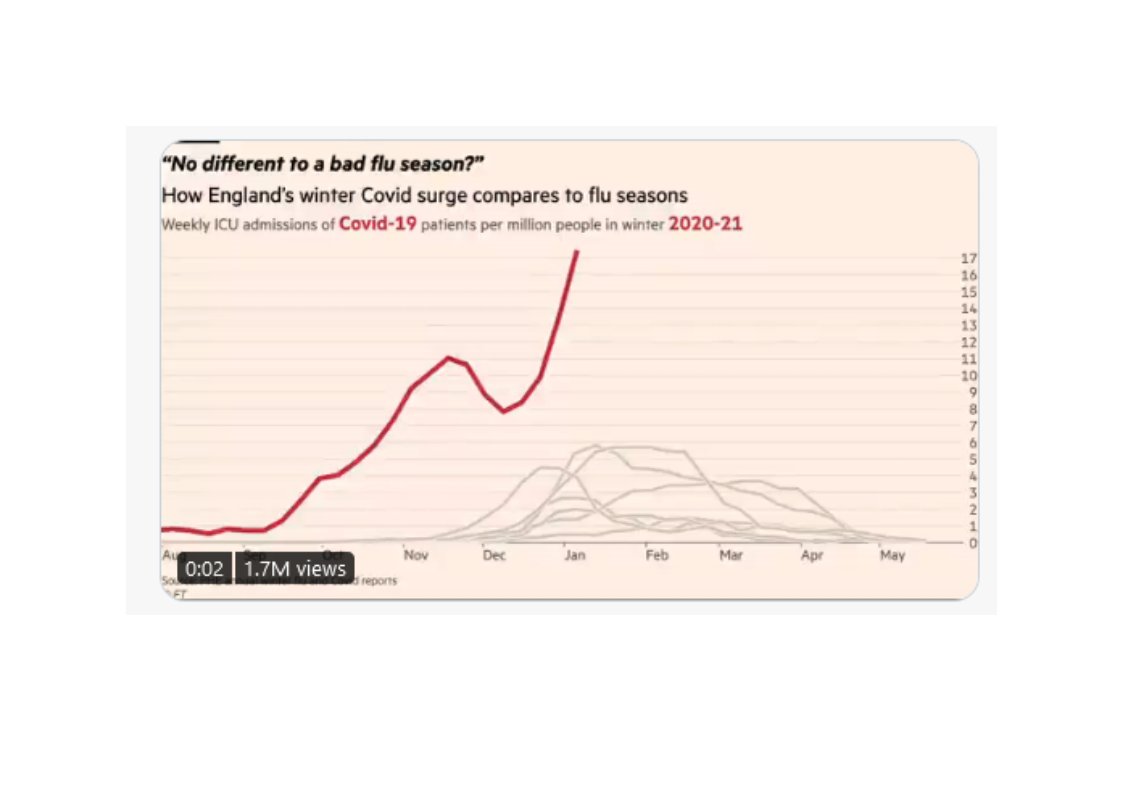
NEW: a common response to reports of hospitals struggling this winter is "it\u2019s no different to a bad flu season!"
— John Burn-Murdoch (@jburnmurdoch) January 7, 2021
I\u2019ve tracked down historical data on flu ICU admissions, including winter 2017-18, a record high.
Here\u2019s how England\u2019s Covid winter compares to a bad flu season \U0001f4f9 pic.twitter.com/tsExrDZM31
Here's a detailed thread explaining how the weekly ONS data should be interpreted when monitoring all cause mortality and excess deaths. It seems very common for people to misinterpret the data relating to excess deaths so I will do my best to clarify in a series of tweets. 1/10 pic.twitter.com/r2TUH7I4wE
— Michael George (@Mike_aka_Logiqx) January 9, 2021
To believe the hypothesis posed by the sceptics you also have to believe this. Either those charged with monitoring the nation\u2019s health \u2013 the CMO, CSA, their colleagues in the regions, Ministers, officials \u2013 are unaware of the data flaws Julia and her allies have identified...
— (((Dan Hodges))) (@DPJHodges) January 8, 2021
More from Health


1/16
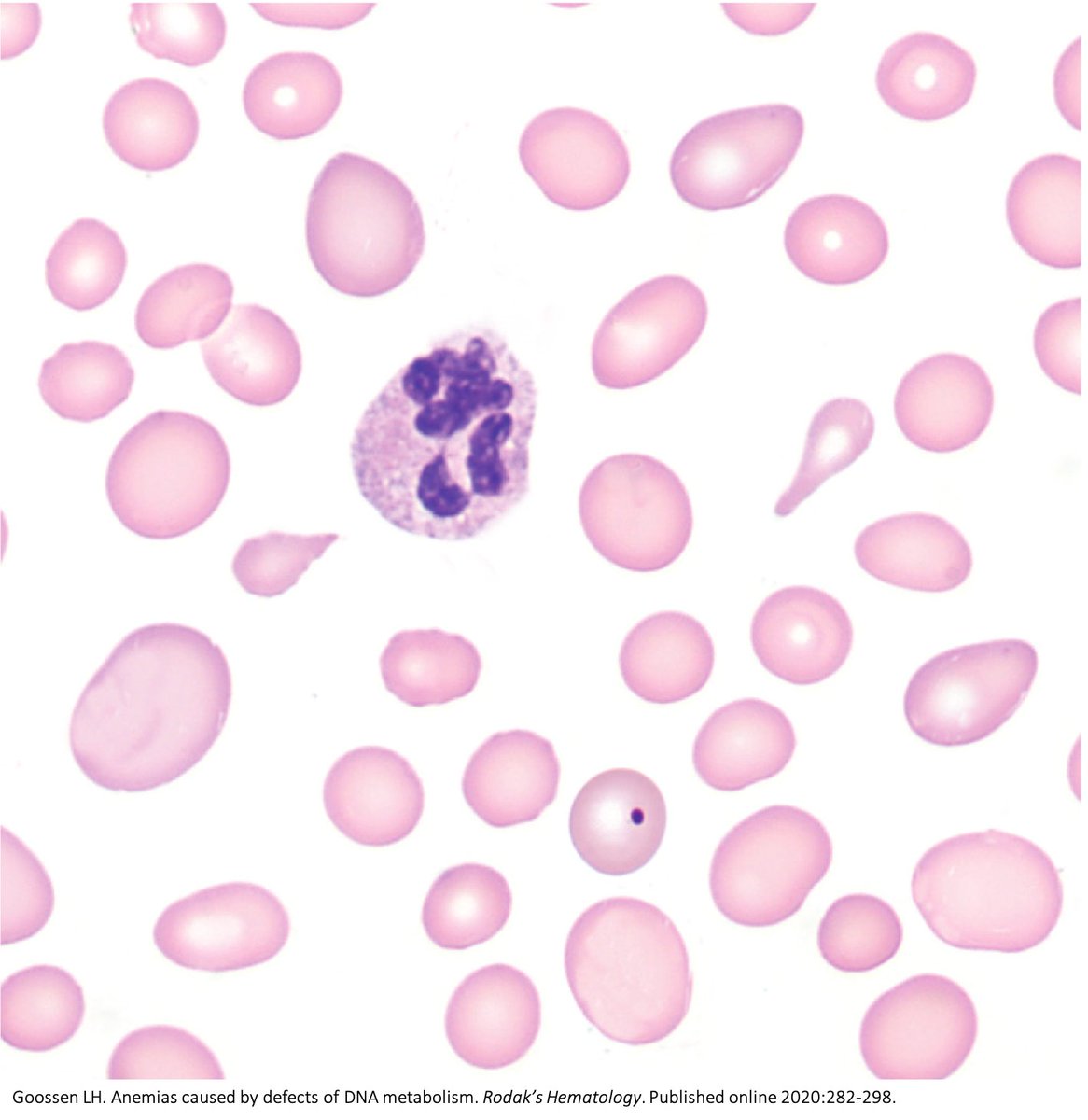
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
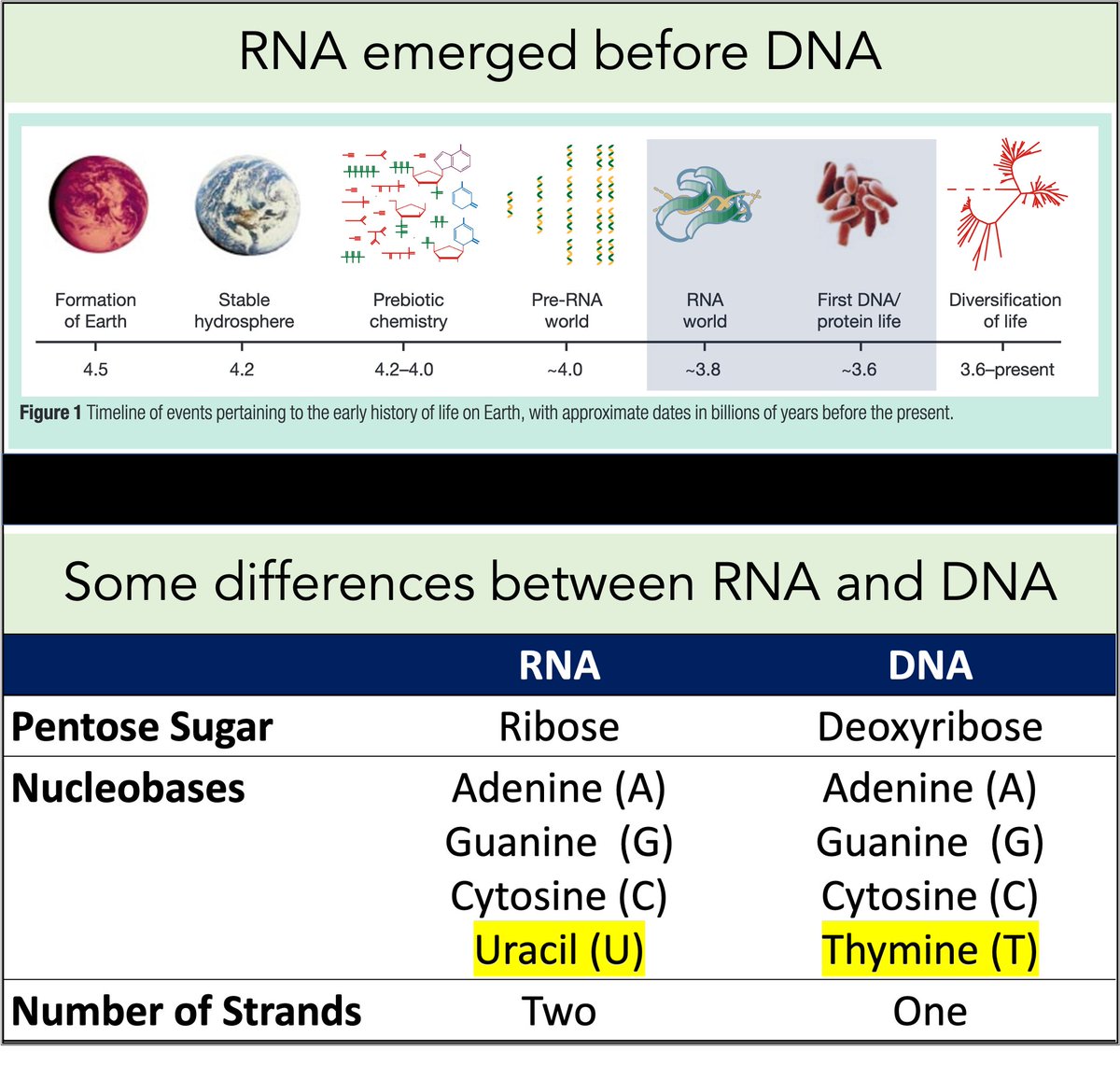
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
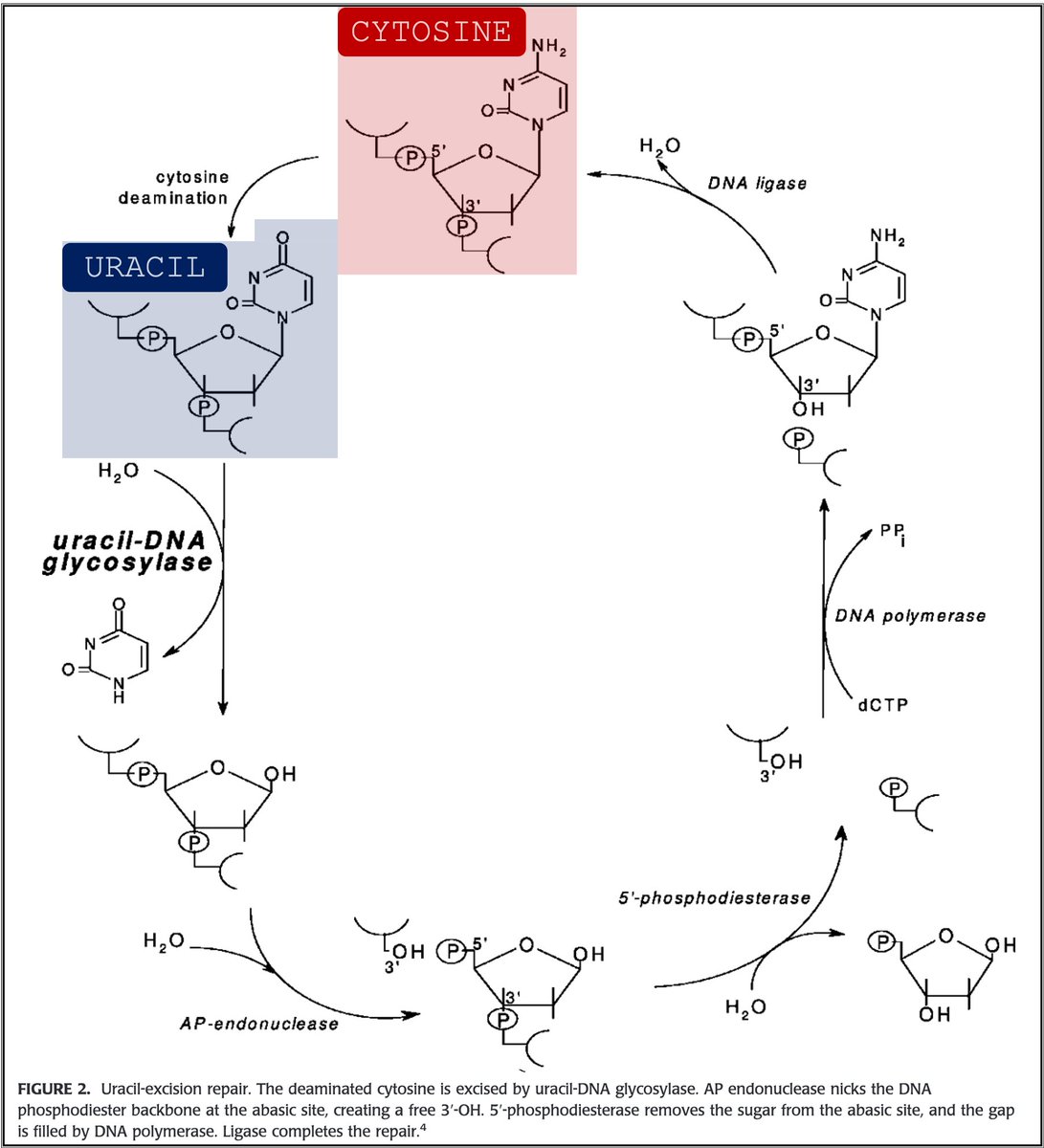
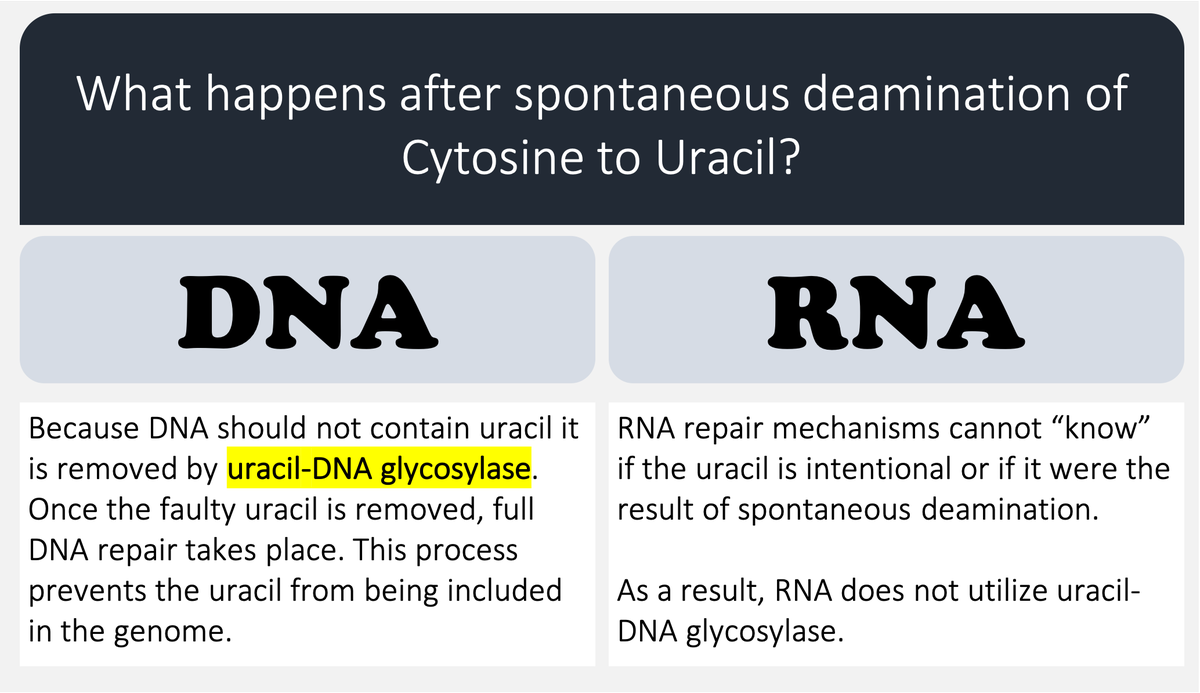
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
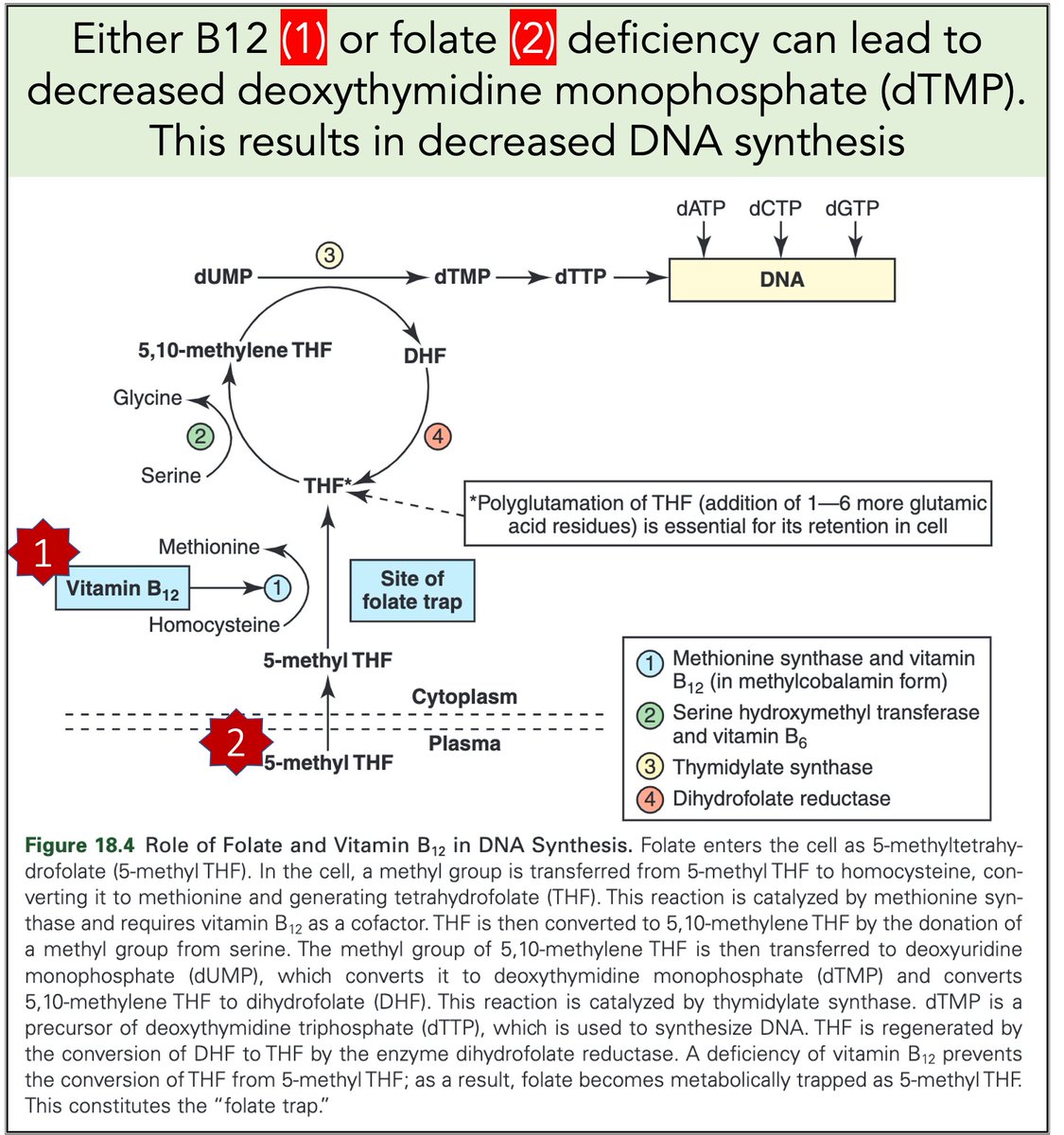
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh






This is the $1mln question still without an answer: why were these workers cleaning bat guano from that abandoned mine?
Surprisingly we simply don't know.
China would have all interest in clarifying that point if for instance they were prospecting or selling guano. It did not.
What we know is that EcoHealth + WIV were sampling bat sites in the vicinity at the exact time of the workers being in that mine.
#DRASTIC wrote about this and about other oddities in the official story:
Maybe it's just one of these coincidences.
Then it gets interesting: about a year after the miners death, Olival & Epstein from EcoHealth Alliance co-authored a paper about the coronavirus risk infection from bat guano collection.
No mention of the
That paper oddly used some old bat samples collected by DARPA in 2006/7 at the famous Thai bat cave.
It never mentioned that the Thai monks have been doing this every Sunday for many many years without infection.
But most interestingly it never mentioned the Mojiang mine accident, even if the perfect timing and recycling of old DARPA bat samples seem to point to a likely knowledge of it.
Anyway, the idea was to ask for more money, as you correctly
Surprisingly we simply don't know.
China would have all interest in clarifying that point if for instance they were prospecting or selling guano. It did not.
The miners were tasked with removing bat feces. AFAIK it hasn't been established why they were doing this. Given that EcoHealth was collecting bat fecal samples in the same province around the same time, is it possible these miners were actually collecting guano for EcoHealth?
— The Great Gumbino (@gumby4christ) February 15, 2021
What we know is that EcoHealth + WIV were sampling bat sites in the vicinity at the exact time of the workers being in that mine.
#DRASTIC wrote about this and about other oddities in the official story:
Maybe it's just one of these coincidences.
Then it gets interesting: about a year after the miners death, Olival & Epstein from EcoHealth Alliance co-authored a paper about the coronavirus risk infection from bat guano collection.
No mention of the
That paper oddly used some old bat samples collected by DARPA in 2006/7 at the famous Thai bat cave.
It never mentioned that the Thai monks have been doing this every Sunday for many many years without infection.
But most interestingly it never mentioned the Mojiang mine accident, even if the perfect timing and recycling of old DARPA bat samples seem to point to a likely knowledge of it.
Anyway, the idea was to ask for more money, as you correctly