
The behaviours of the virus do not depend on the current ‘zone’ of public health restrictions. And, to be perfectly candid, neither should ours. (2/14)
THIS IS A CATCHY & ATTENTION-GRABBING TITLE
Today, the Province will likely announce what zone of the reopening framework we'll shift into as of Tuesday. Whatever is announced, though, doesn't change what we need to do. Why?
Kindly read these 14 tweets & we'll tell you. (1/14)
The behaviours of the virus do not depend on the current ‘zone’ of public health restrictions. And, to be perfectly candid, neither should ours. (2/14)
Nurses, doctors, paramedics & healthcare workers have experienced things much differently than most of us. (3/14)
Business owners & hospitality workers have been on a rollercoaster of openings & closures.
Students, parents, teachers & school staff have had to adapt to going from online (4/14)
And this virus has disproportionately affected some groups more than others.
But there's the thing: while our experiences of this pandemic haven't been shared, we do have a shared goal.
And we can reach it together. (5/14)
Want to help ensure that once our local businesses reopen, they stay open? We can wear masks & physically distance. (6/14)
Helping those who are isolated or have been disproportionately affected? We must get our vaccines when our time comes. (7/14)
Between now and then, we'll be following our COVID-19 Vaccination Plan: https://t.co/WoFmxjyXHW. (8/14)
No one is perfect. In fact, other than the song Tiny Dancer, perfection doesn't exist.
Yes, some of us haven't been 100% #COVIDwise every day. (9/14)
Our actions matter. We know the lack of instant gratification is hard. (10/14)
It's about knowing our actions now will pay dividends later.
And with the new variants, we don't have a choice but to be as vigilant as we can, every day. (11/14)
If you ♥️ or RT this, do it because you're committing. Make it a sign. Your way of saying to your followers that you're on board.
And you won't be alone. (12/14)
More from Health

Now you know I love to sh-t in Harvard. But I also like accuracy. So I decided to go look at Harvard’s catalog to see its lack of military history that this article describes (they only teach history of pets it claims) and what I found shocked me! Shocked me! A thread: 1/
First off, Harvard students literally have multiple sections of military history that they can take listed. (It appears these ones are taught at MIT, so they might have to walk down the street for these) but... 2/

Say they want to stay on campus...they can only take numerous classes on war and diplomacy...3/
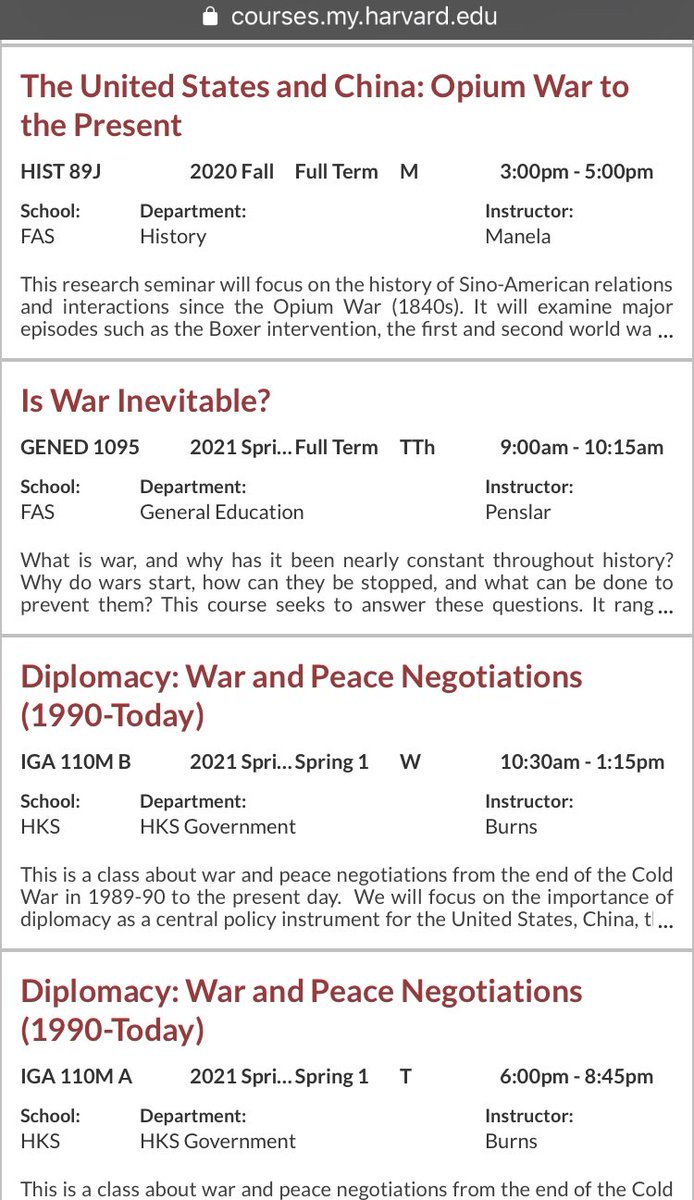
They have an entire class on Yalta. That’s right. An entire class on Yalta. 4/

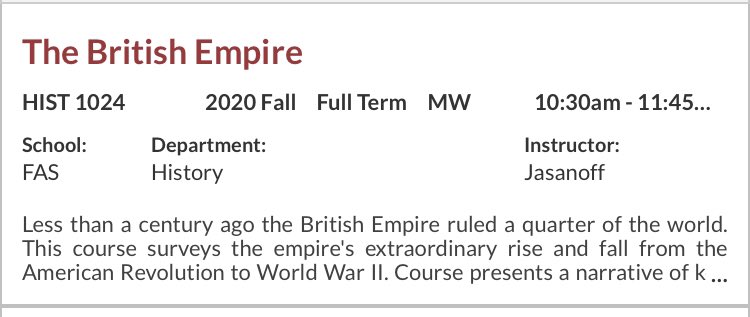
But wait! There is more! They can take the British Empire, The Fall of the Roman Empire for those wanting traditional topics... 5/
\u201cMilitary history\u201d is only in decline if you\u2014like the author & experts in this obnoxious piece\u2014see the subject as a narrowly defined, white dude-oriented, guns & bayonets approach. The field is 1000% better off w/today\u2019s diversity of topics & historians. https://t.co/dUf3OWyVpQ
— Jonathan S. Jones (@_jonathansjones) February 1, 2021
First off, Harvard students literally have multiple sections of military history that they can take listed. (It appears these ones are taught at MIT, so they might have to walk down the street for these) but... 2/
Say they want to stay on campus...they can only take numerous classes on war and diplomacy...3/
They have an entire class on Yalta. That’s right. An entire class on Yalta. 4/
But wait! There is more! They can take the British Empire, The Fall of the Roman Empire for those wanting traditional topics... 5/




You gotta think about this one carefully!
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
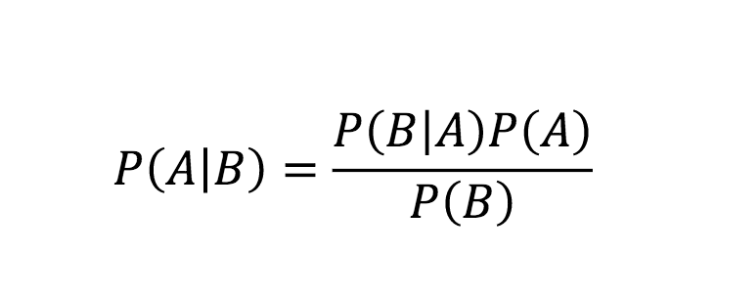
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
Really doesn\u2019t fit well in a tweet. pic.twitter.com/xN0pAyniFS
— Dr. Lena Sugar \U0001f3f3\ufe0f\u200d\U0001f308\U0001f1ea\U0001f1fa\U0001f1ef\U0001f1f5 (@_jvs) February 18, 2021
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇

You May Also Like






**Thread on Bravery of Sikhs**
(I am forced to do this due to continuous hounding of Sikh Extremists since yesterday)
Rani Jindan Kaur, wife of Maharaja Ranjit Singh had illegitimate relations with Lal Singh (PM of Ranjit Singh). Along with Lal Singh, she attacked Jammu, burnt - https://t.co/EfjAq59AyI

Hindu villages of Jasrota, caused rebellion in Jammu, attacked Kishtwar.
Ancestors of Raja Ranjit Singh, The Sansi Tribe used to give daughters as concubines to Jahangir.

The Ludhiana Political Agency (Later NW Fronties Prov) was formed by less than 4000 British soldiers who advanced from Delhi and reached Ludhiana, receiving submissions of all sikh chiefs along the way. The submission of the troops of Raja of Lahore (Ranjit Singh) at Ambala.
Dabistan a contemporary book on Sikh History tells us that Guru Hargobind broke Naina devi Idol Same source describes Guru Hargobind serving a eunuch
YarKhan. (ref was proudly shared by a sikh on twitter)
Gobind Singh followed Bahadur Shah to Deccan to fight for him.

In Zafarnama, Guru Gobind Singh states that the reason he was in conflict with the Hill Rajas was that while they were worshiping idols, while he was an idol-breaker.
And idiot Hindus place him along Maharana, Prithviraj and Shivaji as saviours of Dharma.

(I am forced to do this due to continuous hounding of Sikh Extremists since yesterday)
Rani Jindan Kaur, wife of Maharaja Ranjit Singh had illegitimate relations with Lal Singh (PM of Ranjit Singh). Along with Lal Singh, she attacked Jammu, burnt - https://t.co/EfjAq59AyI
Tomorrow again same thing happens bcoz fudus like you are creating a narrative oh Khalistan. when farmers are asking MSP. (RSS ki tatti khane wale Kerni sena ke kutte).
— Ancient Economist (@_stock_tips) December 5, 2020
U kill sikhs in 1984 just politics. To BC low IQ fudu Saale entire history was politics.
Hindu villages of Jasrota, caused rebellion in Jammu, attacked Kishtwar.
Ancestors of Raja Ranjit Singh, The Sansi Tribe used to give daughters as concubines to Jahangir.
The Ludhiana Political Agency (Later NW Fronties Prov) was formed by less than 4000 British soldiers who advanced from Delhi and reached Ludhiana, receiving submissions of all sikh chiefs along the way. The submission of the troops of Raja of Lahore (Ranjit Singh) at Ambala.
Dabistan a contemporary book on Sikh History tells us that Guru Hargobind broke Naina devi Idol Same source describes Guru Hargobind serving a eunuch
YarKhan. (ref was proudly shared by a sikh on twitter)
Gobind Singh followed Bahadur Shah to Deccan to fight for him.
In Zafarnama, Guru Gobind Singh states that the reason he was in conflict with the Hill Rajas was that while they were worshiping idols, while he was an idol-breaker.
And idiot Hindus place him along Maharana, Prithviraj and Shivaji as saviours of Dharma.