
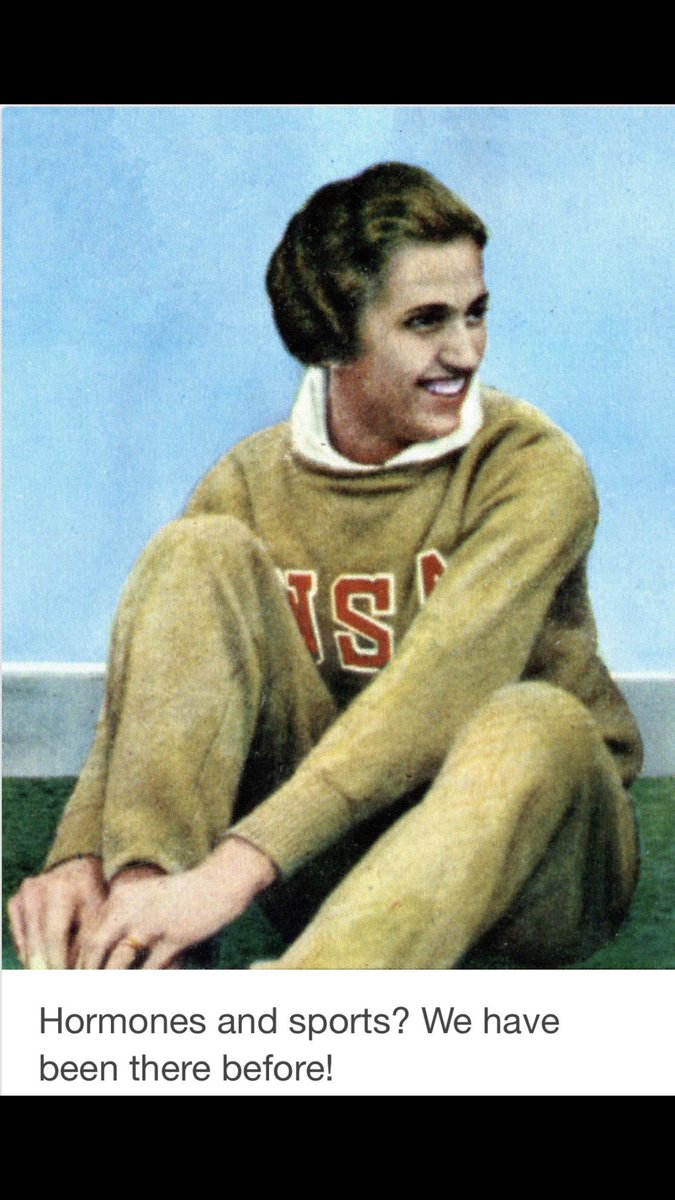
How long should trans females be made to reduce their levels of circulating testosterone should prior to competing in the women competition?

https://t.co/MOZtfh5Raf
https://t.co/8rMfUi4brV
https://t.co/0SqyneBjPZ…
https://t.co/pgyggiNG2u
https://t.co/0SqyneBjPZ…
https://t.co/A5AVkkShDj
https://t.co/S2yyg9Xq8j
https://t.co/Bcg0PuNNu3
https://t.co/Bcg0PuNNu3
https://t.co/2bii5lMZYy
https://t.co/olda0NryXA

End
More from Kirsti Miller


There is little understanding within Australian society of the requirement to and legitimacy of adopting special measures.
Government policy does not acknowledge the applicability to Indigenous people of the right to self-determination. In 1997 the cruel Howard government actively rejected self- determination as the basis of Indigenous policy.
Key reports which make recommendations for redressing Indigenous disadvantage, including the Royal Commission into Aboriginal Deaths in Custody, and Bringing them home, .....
the National Inquiry into the Separation of Aboriginal and Torres Strait Islander Children from Their Families, have ’NOT’ been fully implemented.
Many recommendations, particularly those concerning the application of the principle of self-determination, have been actively rejected.
Such a waste
— Steve Grey (@Stephen_J_Grey) January 28, 2021
Government policy does not acknowledge the applicability to Indigenous people of the right to self-determination. In 1997 the cruel Howard government actively rejected self- determination as the basis of Indigenous policy.
Key reports which make recommendations for redressing Indigenous disadvantage, including the Royal Commission into Aboriginal Deaths in Custody, and Bringing them home, .....
the National Inquiry into the Separation of Aboriginal and Torres Strait Islander Children from Their Families, have ’NOT’ been fully implemented.
Many recommendations, particularly those concerning the application of the principle of self-determination, have been actively rejected.

More from Society

A long thread on how an obsessive & violent antisemite & Holocaust denier has been embraced by the international “community of the good.”
Sarah Wilkinson has a history of Holocaust denial & anti-Jewish hatred dating back (in documented examples) to around 2015.

She is a self-proclaimed British activist for “Palestinian rights” but is more accurately a far Left neo-Nazi. Her son shares the same characteristics of violence, racism & Holocaust denial.
I first documented Sarah Wilkinson’s Holocaust denial back in July 2016. I believe I was the 1st person to do so.
Since then she has produced a long trail of written hate and abuse. See here for a good summary.
Wilkinson has recently been publicly celebrated by @XRebellionUK over her latest violent action against a Jewish owned business. Despite many people calling XR’s attention to her history, XR have chosen to remain in alliance with this neo-Nazi.
Former Labour Shadow Chancellor John McDonnell MP is among those who also chose to stand with Wilkinson via a tweet.
But McDonnell is not alone.
Neo-Nazi Sarah Wilkinson is supported and encouraged by thousands of those on the Left who consider themselves “anti-racists”.
Sarah Wilkinson has a history of Holocaust denial & anti-Jewish hatred dating back (in documented examples) to around 2015.
She is a self-proclaimed British activist for “Palestinian rights” but is more accurately a far Left neo-Nazi. Her son shares the same characteristics of violence, racism & Holocaust denial.
I first documented Sarah Wilkinson’s Holocaust denial back in July 2016. I believe I was the 1st person to do so.
Since then she has produced a long trail of written hate and abuse. See here for a good summary.
The internet is forever. https://t.co/zxBV7rjskB
— Heidi Bachram (@HeidiBachram) February 2, 2021
Wilkinson has recently been publicly celebrated by @XRebellionUK over her latest violent action against a Jewish owned business. Despite many people calling XR’s attention to her history, XR have chosen to remain in alliance with this neo-Nazi.
Former Labour Shadow Chancellor John McDonnell MP is among those who also chose to stand with Wilkinson via a tweet.
But McDonnell is not alone.
Neo-Nazi Sarah Wilkinson is supported and encouraged by thousands of those on the Left who consider themselves “anti-racists”.






The Nashville Operation - A Battle in the War
A thread exploring the Nashville bombing in the context of the 2020 Digital War (via SolarWinds) against the United States perpetrated by our enemies, likely China, Iran and/or Russia.

SolarWinds Hack
A digital "Pearl Harbor" moment for the United States, whoever was responsible had access to the keys to the kingdom for months during 2020, including sensitive military infrastructure. This is war!
SunGard + SolarWinds
SolarWinds software company is owned by same company that owns SunGard, which essentially provides data center services. A secure place to host internet servers with redundant power and "big pipe" data connections.
https://t.co/U3P3SrrkM1

SunGard Data Center
In Nashville, around the corner from their "big pipe" connection, AT&T. Like any data center, highly secure. Only authorized personnel can enter, and even fewer can access the actual server rooms. Backup generators are available in case of power failure.

If the SunGard hardware was being used to "host" critical command and control software related to SolarWinds, the US powers would be very interested in gaining special access keys that are stored on the hard-drives of specific servers.

A thread exploring the Nashville bombing in the context of the 2020 Digital War (via SolarWinds) against the United States perpetrated by our enemies, likely China, Iran and/or Russia.
SolarWinds Hack
A digital "Pearl Harbor" moment for the United States, whoever was responsible had access to the keys to the kingdom for months during 2020, including sensitive military infrastructure. This is war!
SunGard + SolarWinds
SolarWinds software company is owned by same company that owns SunGard, which essentially provides data center services. A secure place to host internet servers with redundant power and "big pipe" data connections.
https://t.co/U3P3SrrkM1
SunGard Data Center
In Nashville, around the corner from their "big pipe" connection, AT&T. Like any data center, highly secure. Only authorized personnel can enter, and even fewer can access the actual server rooms. Backup generators are available in case of power failure.
If the SunGard hardware was being used to "host" critical command and control software related to SolarWinds, the US powers would be very interested in gaining special access keys that are stored on the hard-drives of specific servers.

Hi @officestudents @EHRC @EHRCChair @KishwerFalkner @RJHilsenrath @trussliz @GEOgovuk
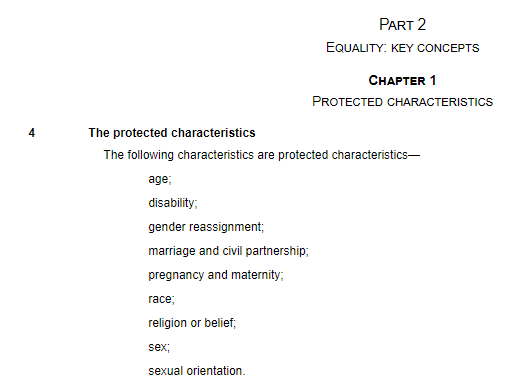
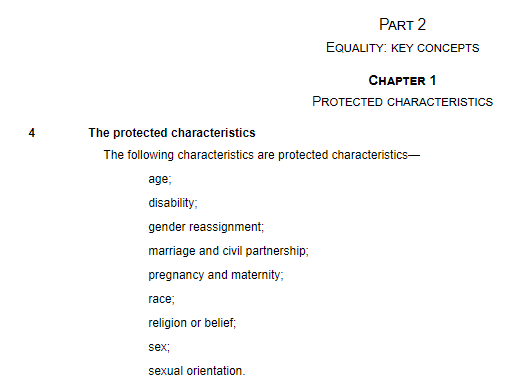
The Equality and Diversity section of your job application has 'gender' in what appears to be a list of the protected characteristics under the Equality Act 2010.
However...
1/15
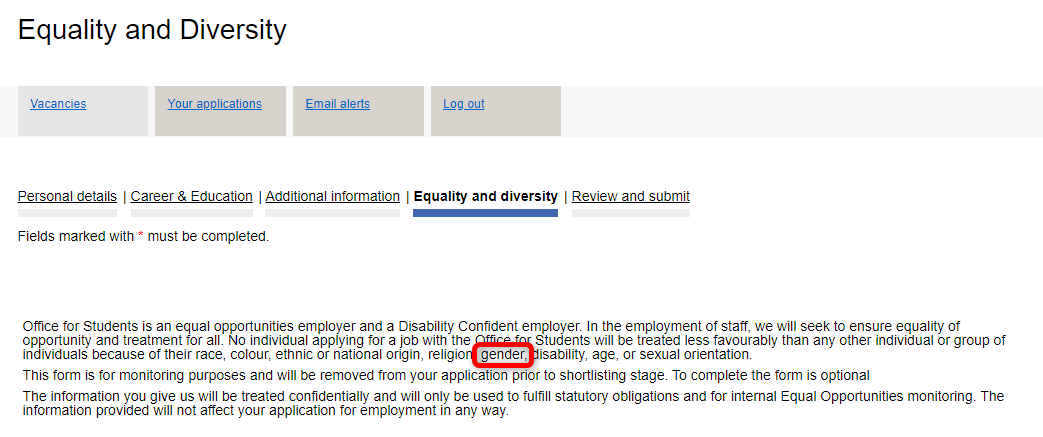
However, 'gender' is not a protected characteristic under the Equality Act 2010 and is not defined in the Act.
https://t.co/qisFhCiV1u
Sex is the protected characteristic under the Act, but that is not on your list.
2/15
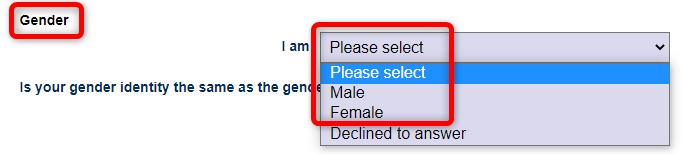
You then ask for the 'gender' of the applicant with options:
Male
Female.
3/15
Again, 'gender' is not a protected characteristic under the Equality Act 2010 and is not defined in the Act.
https://t.co/qisFhCiV1u
4/15
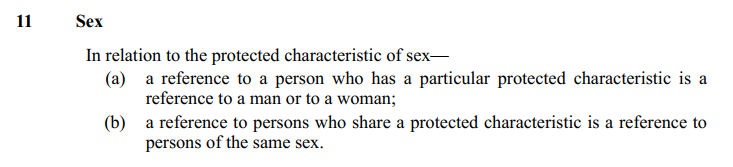
Sex is the protected characteristic and the only two possible options for sex are 'Female' and 'Male' as defined in the Act and consistent with biology, but you don't ask for that.
https://t.co/CEJ0gkr6nF
'Gender' is not a synonym for sex.
5/15
The Equality and Diversity section of your job application has 'gender' in what appears to be a list of the protected characteristics under the Equality Act 2010.
However...
1/15
However, 'gender' is not a protected characteristic under the Equality Act 2010 and is not defined in the Act.
https://t.co/qisFhCiV1u
Sex is the protected characteristic under the Act, but that is not on your list.
2/15
You then ask for the 'gender' of the applicant with options:
Male
Female.
3/15
Again, 'gender' is not a protected characteristic under the Equality Act 2010 and is not defined in the Act.
https://t.co/qisFhCiV1u
4/15
Sex is the protected characteristic and the only two possible options for sex are 'Female' and 'Male' as defined in the Act and consistent with biology, but you don't ask for that.
https://t.co/CEJ0gkr6nF
'Gender' is not a synonym for sex.
5/15

You May Also Like

I think a plausible explanation is that whatever Corbyn says or does, his critics will denounce - no matter how much hypocrisy it necessitates.
Corbyn opposes the exploitation of foreign sweatshop-workers - Labour MPs complain he's like Nigel
He speaks up in defence of migrants - Labour MPs whinge that he's not listening to the public's very real concerns about immigration:
He's wrong to prioritise Labour Party members over the public:
He's wrong to prioritise the public over Labour Party
One of the oddest features of the Labour tax row is how raising allowances, which the media allowed the LDs to describe as progressive (in spite of evidence to contrary) through the coalition years, is now seen by everyone as very right wing
— Tom Clark (@prospect_clark) November 2, 2018
Corbyn opposes the exploitation of foreign sweatshop-workers - Labour MPs complain he's like Nigel
He speaks up in defence of migrants - Labour MPs whinge that he's not listening to the public's very real concerns about immigration:
He's wrong to prioritise Labour Party members over the public:
He's wrong to prioritise the public over Labour Party

1/Politics thread time.
To me, the most important aspect of the 2018 midterms wasn't even about partisan control, but about democracy and voting rights. That's the real battle.
2/The good news: It's now an issue that everyone's talking about, and that everyone cares about.
3/More good news: Florida's proposition to give felons voting rights won. But it didn't just win - it won with substantial support from Republican voters.
That suggests there is still SOME grassroots support for democracy that transcends
4/Yet more good news: Michigan made it easier to vote. Again, by plebiscite, showing broad support for voting rights as an
5/OK, now the bad news.
We seem to have accepted electoral dysfunction in Florida as a permanent thing. The 2000 election has never really
To me, the most important aspect of the 2018 midterms wasn't even about partisan control, but about democracy and voting rights. That's the real battle.
2/The good news: It's now an issue that everyone's talking about, and that everyone cares about.
3/More good news: Florida's proposition to give felons voting rights won. But it didn't just win - it won with substantial support from Republican voters.
That suggests there is still SOME grassroots support for democracy that transcends
4/Yet more good news: Michigan made it easier to vote. Again, by plebiscite, showing broad support for voting rights as an
5/OK, now the bad news.
We seem to have accepted electoral dysfunction in Florida as a permanent thing. The 2000 election has never really
Bad ballot design led to a lot of undervotes for Bill Nelson in Broward Co., possibly even enough to cost him his Senate seat. They do appear to be real undervotes, though, instead of tabulation errors. He doesn't really seem to have a path to victory. https://t.co/utUhY2KTaR
— Nate Silver (@NateSilver538) November 16, 2018






MDZS is laden with buddhist references. As a South Asian person, and history buff, it is so interesting to see how Buddhism, which originated from India, migrated, flourished & changed in the context of China. Here's some research (🙏🏼 @starkjeon for CN insight + citations)
1. LWJ’s sword Bichen ‘is likely an abbreviation for the term 躲避红尘 (duǒ bì hóng chén), which can be translated as such: 躲避: shunning or hiding away from 红尘 (worldly affairs; which is a buddhist teaching.) (https://t.co/zF65W3roJe) (abbrev. TWX)
2. Sandu (三 毒), Jiang Cheng’s sword, refers to the three poisons (triviṣa) in Buddhism; desire (kāma-taṇhā), delusion (bhava-taṇhā) and hatred (vibhava-taṇhā).
These 3 poisons represent the roots of craving (tanha) and are the cause of Dukkha (suffering, pain) and thus result in rebirth.
Interesting that MXTX used this name for one of the characters who suffers, arguably, the worst of these three emotions.
3. The Qian kun purse “乾坤袋 (qián kūn dài) – can be called “Heaven and Earth” Pouch. In Buddhism, Maitreya (मैत्रेय) owns this to store items. It was believed that there was a mythical space inside the bag that could absorb the world.” (TWX)
1. LWJ’s sword Bichen ‘is likely an abbreviation for the term 躲避红尘 (duǒ bì hóng chén), which can be translated as such: 躲避: shunning or hiding away from 红尘 (worldly affairs; which is a buddhist teaching.) (https://t.co/zF65W3roJe) (abbrev. TWX)
2. Sandu (三 毒), Jiang Cheng’s sword, refers to the three poisons (triviṣa) in Buddhism; desire (kāma-taṇhā), delusion (bhava-taṇhā) and hatred (vibhava-taṇhā).
These 3 poisons represent the roots of craving (tanha) and are the cause of Dukkha (suffering, pain) and thus result in rebirth.
Interesting that MXTX used this name for one of the characters who suffers, arguably, the worst of these three emotions.
3. The Qian kun purse “乾坤袋 (qián kūn dài) – can be called “Heaven and Earth” Pouch. In Buddhism, Maitreya (मैत्रेय) owns this to store items. It was believed that there was a mythical space inside the bag that could absorb the world.” (TWX)