
THREAD: Women and "Unexplained" Diseases
It's interesting that even a condition as common as #Migraine is still not well understood.
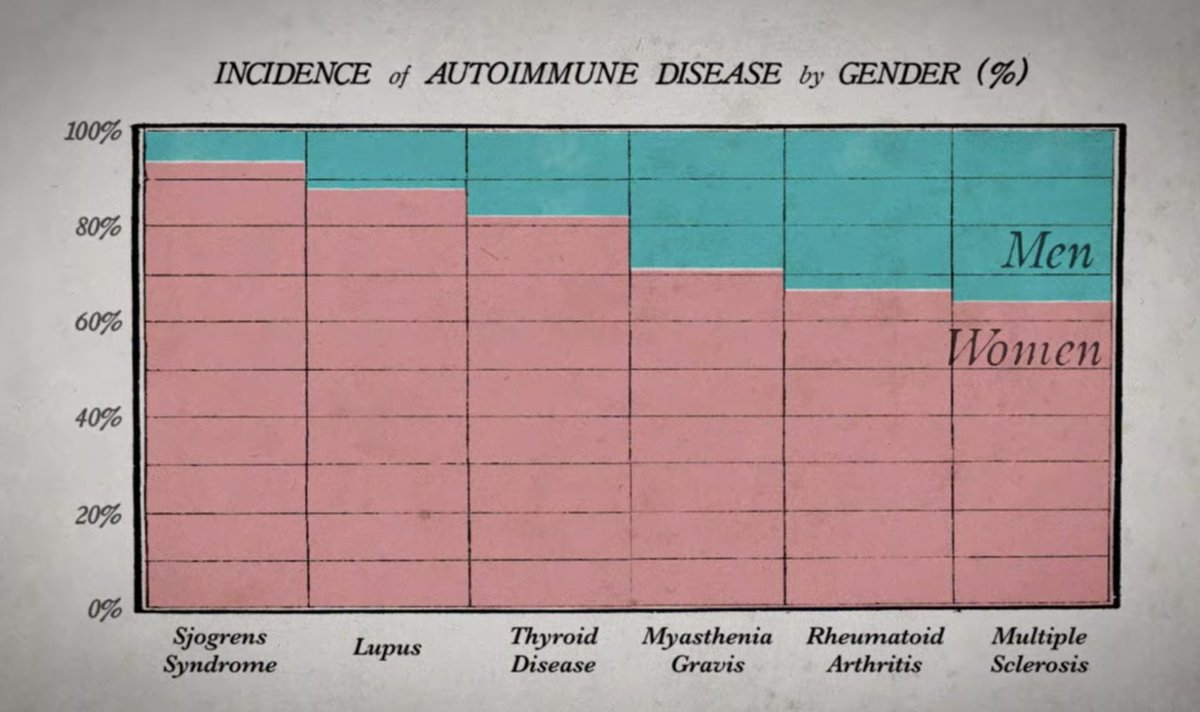
Significant overlap with many other conditions mostly impacting women that are also "not well understood" is present.
https://t.co/EhrnxfItsm https://t.co/R7QUKrZvhR
cc: @jenbrea @ahandvanish @AthenaAkrami @Dr2NisreenAlwan @MBVanElzakker
https://t.co/ITrLBkc3uE
If you work on #longCOVID and say \u201cI\u2019m not an #MECFS expert, I don\u2019t know anything about it, it\u2019s not my job to know about ME or \u2019fatigue\u2019\u201d then you really, REALLY need to learn about ME. This is what MANY infections can do, not just SARS2. pic.twitter.com/zke0MqwrEd
— Jennifer Brea\U0001f992 (@jenbrea) January 14, 2021
Example stats ME/CFS:
https://t.co/GKQqqtWTI7
In ME/CFS is about 80/20 female/male. Before puberty, gender ratio is 50/50. Many anecdotal reports of trans people who take hormones: F to M improve, M to F experience worsening symptoms. Female preponderance is found in both sporadic cases and historically, in outbreaks.
— Jennifer Brea\U0001f992 (@jenbrea) January 12, 2021
Majority of patients with PNES are women, outnumbering men by a ratio of 3:1. Female sex preponderance occurs after puberty & usually before the age of 55
Lack of data does not equal lack of EXISTENCE of a problem, it equals lack of UNDERSTANDING of the problem.
And this problem is immense.
https://t.co/TnF2j4dKs3
Like this tweet if:
— Dr. Jessica Taylor (@DrJessTaylor) January 13, 2021
- You are a woman
- You have ever been ignored, gaslit, accused of exaggerating or told its all in your head by a doctor when you sought help for a medical problem
I just wanna see something.
My optimistic hope is that the enormous amounts of funding for #COVID19 open doors to understanding pathophysiology of previously neglected diseases particularly in women.
But our scientific ignorance should not be wielded to blame & further abuse patients.
Our lack of understanding is not their failure but ours.
https://t.co/LwN8qc0Q4a
Well, it would be so much easier if we didn\u2019t continuously \u201ccarve diagnoses out of the psychosomatic wastebasket\u201d as Maya Dusenbury so eloquently wrote in her book Doing Harm. So I will continue to rant about it. Wont make the medical profession happy, but time to face reality... pic.twitter.com/iFJudV9BLX
— GinaMcGalliard \U0001f9dc\U0001f3fb\u200d\u2640\ufe0f\U0001f315\U0001f339 (@GinaMcGalliard) January 12, 2021
There are more specific, more scientific, and less offensive terminology we can use for women's bodies.
@VirusesImmunity @angie_rasmussen @DocElovitz
To read more of my Threads, please check out: https://t.co/UMdZvE2tDj
More from Health


Public Health Scholarships
This may help for those considering MS/PhD in Public Health
1. The Erasmus Mundus Joint Master Degree in Public Health in Disasters
https://t.co/1Z5qpstsSu
2. Afya Bora Global Health
3. Carl Duisberg Scholarships
https://t.co/HnNXdbWBxy
4. Commonwealth Scholarships for Developing Countries
https://t.co/3fWGf5b2OH
5. Fellowships in Public Health & Tropical
6. Fellowships to Promote Mental Health Journalism
https://t.co/MVV9PFsBJ1
7. 2021-22 Jeroen Ensink Memorial Fund
8. Paul S. Lietman Global Travel Grant for Residents & Fellows
https://t.co/qK76R495QT
9. Global Health Internships and Funding
https://t.co/FD9Gh2wXvO
10. Kofi Annan Global Health Leadership
11. MA in European Public Health
https://t.co/5x0Vr7b1j8
12. MSc in Public Health Scholarships - Maastricht University,
This may help for those considering MS/PhD in Public Health
1. The Erasmus Mundus Joint Master Degree in Public Health in Disasters
https://t.co/1Z5qpstsSu
2. Afya Bora Global Health
3. Carl Duisberg Scholarships
https://t.co/HnNXdbWBxy
4. Commonwealth Scholarships for Developing Countries
https://t.co/3fWGf5b2OH
5. Fellowships in Public Health & Tropical
6. Fellowships to Promote Mental Health Journalism
https://t.co/MVV9PFsBJ1
7. 2021-22 Jeroen Ensink Memorial Fund
8. Paul S. Lietman Global Travel Grant for Residents & Fellows
https://t.co/qK76R495QT
9. Global Health Internships and Funding
https://t.co/FD9Gh2wXvO
10. Kofi Annan Global Health Leadership
11. MA in European Public Health
https://t.co/5x0Vr7b1j8
12. MSc in Public Health Scholarships - Maastricht University,




Some thoughts on this: Firstly, it might be personal preference, but I am not keen on this kind of campaign as I feel like it trivialises cancer. Sometimes the serious message gets lost because people are sharing pics of cats or whatever and the important context is gone.
More importantly, the statistic being used in the campaign is misleading. It says 57% of women put off cervical screening if they can't get waxed. But on further investigation, that's not accurate.
The page here goes on to say "57% of women who regularly have their pubic hair professionally removed would put off attending their cervical screening appointment if they hadn’t been able to visit a beauty salon."
So the 57% represents a concern not across the whole population of women, but only those who regularly get waxed. So how big of an issue is this across the whole population? And what else is stopping people getting smears?
I think campaigns for cancer screening are really tricky because there is so much nuance that often doesn't fit into a catchy headline or hashtag. It's certainly not easy and is part of a bigger conversation.
It\u2019s #CervicalCancerPreventionWeek \U0001f499
— myGP (@myGPapp) January 18, 2021
Here\u2019s how you can help to raise awareness:
\U0001f431 Share an image of the cat that best reflects your undercarriage/flower/bits (technical term vulva!) current look.
#\u20e3Use the Hashtag #myCat.
\U0001f46dTell and tag your friends to let them know. pic.twitter.com/8aHf96ynjT
More importantly, the statistic being used in the campaign is misleading. It says 57% of women put off cervical screening if they can't get waxed. But on further investigation, that's not accurate.
The page here goes on to say "57% of women who regularly have their pubic hair professionally removed would put off attending their cervical screening appointment if they hadn’t been able to visit a beauty salon."
So the 57% represents a concern not across the whole population of women, but only those who regularly get waxed. So how big of an issue is this across the whole population? And what else is stopping people getting smears?
I think campaigns for cancer screening are really tricky because there is so much nuance that often doesn't fit into a catchy headline or hashtag. It's certainly not easy and is part of a bigger conversation.
You May Also Like



The YouTube algorithm that I helped build in 2011 still recommends the flat earth theory by the *hundreds of millions*. This investigation by @RawStory shows some of the real-life consequences of this badly designed AI.
This spring at SxSW, @SusanWojcicki promised "Wikipedia snippets" on debated videos. But they didn't put them on flat earth videos, and instead @YouTube is promoting merchandising such as "NASA lies - Never Trust a Snake". 2/

A few example of flat earth videos that were promoted by YouTube #today:
https://t.co/TumQiX2tlj 3/
https://t.co/uAORIJ5BYX 4/
https://t.co/yOGZ0pLfHG 5/
Flat Earth conference attendees explain how they have been brainwashed by YouTube and Infowarshttps://t.co/gqZwGXPOoc
— Raw Story (@RawStory) November 18, 2018
This spring at SxSW, @SusanWojcicki promised "Wikipedia snippets" on debated videos. But they didn't put them on flat earth videos, and instead @YouTube is promoting merchandising such as "NASA lies - Never Trust a Snake". 2/
A few example of flat earth videos that were promoted by YouTube #today:
https://t.co/TumQiX2tlj 3/
https://t.co/uAORIJ5BYX 4/
https://t.co/yOGZ0pLfHG 5/

A THREAD ON @SarangSood
Decoded his way of analysis/logics for everyone to easily understand.
Have covered:
1. Analysis of volatility, how to foresee/signs.
2. Workbook
3. When to sell options
4. Diff category of days
5. How movement of option prices tell us what will happen
1. Keeps following volatility super closely.
Makes 7-8 different strategies to give him a sense of what's going on.
Whichever gives highest profit he trades in.
2. Theta falls when market moves.
Falls where market is headed towards not on our original position.
3. If you're an options seller then sell only when volatility is dropping, there is a high probability of you making the right trade and getting profit as a result
He believes in a market operator, if market mover sells volatility Sarang Sir joins him.
4. Theta decay vs Fall in vega
Sell when Vega is falling rather than for theta decay. You won't be trapped and higher probability of making profit.
Decoded his way of analysis/logics for everyone to easily understand.
Have covered:
1. Analysis of volatility, how to foresee/signs.
2. Workbook
3. When to sell options
4. Diff category of days
5. How movement of option prices tell us what will happen
1. Keeps following volatility super closely.
Makes 7-8 different strategies to give him a sense of what's going on.
Whichever gives highest profit he trades in.
I am quite different from your style. I follow the market's volatility very closely. I have mock positions in 7-8 different strategies which allows me to stay connected. Whichever gives best profit is usually the one i trade in.
— Sarang Sood (@SarangSood) August 13, 2019
2. Theta falls when market moves.
Falls where market is headed towards not on our original position.
Anilji most of the time these days Theta only falls when market moves. So the Theta actually falls where market has moved to, not where our position was in the first place. By shifting we can come close to capturing the Theta fall but not always.
— Sarang Sood (@SarangSood) June 24, 2019
3. If you're an options seller then sell only when volatility is dropping, there is a high probability of you making the right trade and getting profit as a result
He believes in a market operator, if market mover sells volatility Sarang Sir joins him.
This week has been great so far. The main aim is to be in the right side of the volatility, rest the market will reward.
— Sarang Sood (@SarangSood) July 3, 2019
4. Theta decay vs Fall in vega
Sell when Vega is falling rather than for theta decay. You won't be trapped and higher probability of making profit.
There is a difference between theta decay & fall in vega. Decay is certain but there is no guaranteed profit as delta moves can increase cost. Fall in vega on the other hand is backed by a powerful force that sells options and gives handsome returns. Our job is to identify them.
— Sarang Sood (@SarangSood) February 12, 2020





