NEW—CDC was truly suffocated by Trump WH at every turn. Kyle McGowan, a former chief of staff at CDC, and his deputy, Amanda Campbell, witnessed WH dismissal of science, WH’s slow suffocation of CDC’s voice, meddling in messages & siphoning of CDC budget.
https://t.co/HeuNbUggiw

Mr. McGowan recalled a White House fixated on the economic implications of public health.
They compromised anyway, recommending social distancing without a reference to the typical six-foot measurement.
“What’s not legitimate is to overrule science,” he said.
(Sidebar: Dr Messonier is my hero)
“They need to be allowed to lead.”
➡️ all this is incredible painful to me cuz of what I also went thru in Jan trying to warn:
https://t.co/I5G7PL6boG
More from Eric Feigl-Ding

📍DOUBLE REINFECTIONS—wow, both PM Justin Trudeau and Biden’s HHS Secretary Becerra got *reinfected* with #COVID19–from same conference—➡️when did Becerra last get infected? May 18th 2022—not even a full month ago! Trudeau in Jan 2022. I worry it’s reinfections due to #BA5/#BA4.
2) #BA5 and #BA4 are worrisome. They are surging and they have high reinfection potential. Your past BA1/BA2 doesn’t substantially protect you from #Ba5/4
3) Excess deaths—the new #BA4 & #BA5 variants of the coronavirus are currently the **fastest growing** strains in the US & UK. ➡️They are exponentially replacing all other past strains. Learn from South Africa’s early warning signs and their excess deaths. #CovidIsNotOver #COVID
4) Is it a Paxlovid rebound for Becerra, as some are asking? Unclear—Paxlovid rebound usually only happens at day 10-14 that we know of and have data. The FDA says it’s 1-2% rebound but I counted 12% from this Pfizer graph submitted to FDA.
5) and yes, #ba5 / #BA4 are very problematic. they are 2x more resistant than even BA2 for neutralizing the virus compared to those who had breakthrough reinfections from older Omicron.
HHS @SecBecerra has tested positive for COVID-19 again, the agency just announced. Last time he tested positive was May 18, after attending the G-7 Summit.
— Ariel Cohen (@ArielCohen37) June 13, 2022
2) #BA5 and #BA4 are worrisome. They are surging and they have high reinfection potential. Your past BA1/BA2 doesn’t substantially protect you from #Ba5/4
\U0001f4c8Surging #BA5 & #BA4 variants in both US & England. It\u2019s looking like #Ba5 is the new fastest strain\u2014which has ~10x increased in England in 1 month. Also notice that older #Omicron #B11529/#BA1 are already near *extinct*. I worry the \u201cnew\u201d Omicron BA1 bivalent vaccine is behind. pic.twitter.com/kLNH0gzPk3
— Eric Feigl-Ding (@DrEricDing) June 9, 2022
3) Excess deaths—the new #BA4 & #BA5 variants of the coronavirus are currently the **fastest growing** strains in the US & UK. ➡️They are exponentially replacing all other past strains. Learn from South Africa’s early warning signs and their excess deaths. #CovidIsNotOver #COVID
To anyone pointing to South Africa to suggest the impact of the omicron wave has been 'mild' or that the BA.4/5 haven't had much impact, I'd urge you to look at excess deaths. 29,500 excess deaths since Jan (omicron wave) & a peak of 1,844 excess deaths/wk during BA.4/5 wave.\U0001f9f5 pic.twitter.com/r7kLzmD5dG
— Dr. Deepti Gurdasani (@dgurdasani1) June 11, 2022
4) Is it a Paxlovid rebound for Becerra, as some are asking? Unclear—Paxlovid rebound usually only happens at day 10-14 that we know of and have data. The FDA says it’s 1-2% rebound but I counted 12% from this Pfizer graph submitted to FDA.
4) Look at these 97 Paxlovid patients here with viral RNA load data over time. Of 97, i conservatively counted at least 12 of 97 (12%) with viral load rebound after day 10. Even more if you count rebound after day 5. Thus, FDA\u2019s 1-2% doesn\u2019t match up here. https://t.co/bNoqj5W3Sk pic.twitter.com/B3Kh0Lc1A4
— Eric Feigl-Ding (@DrEricDing) May 5, 2022
5) and yes, #ba5 / #BA4 are very problematic. they are 2x more resistant than even BA2 for neutralizing the virus compared to those who had breakthrough reinfections from older Omicron.
Unfortunately neutralization experiments found that BA.4/5 is 2x more resistant than BA.2 to the blood obtained from vaccinated individuals who had a breakthrough infection with BA.1 or BA.2. 4/ pic.twitter.com/MEOPXuqTgg
— Dr. Jeff Gilchrist (@jeffgilchrist) June 13, 2022
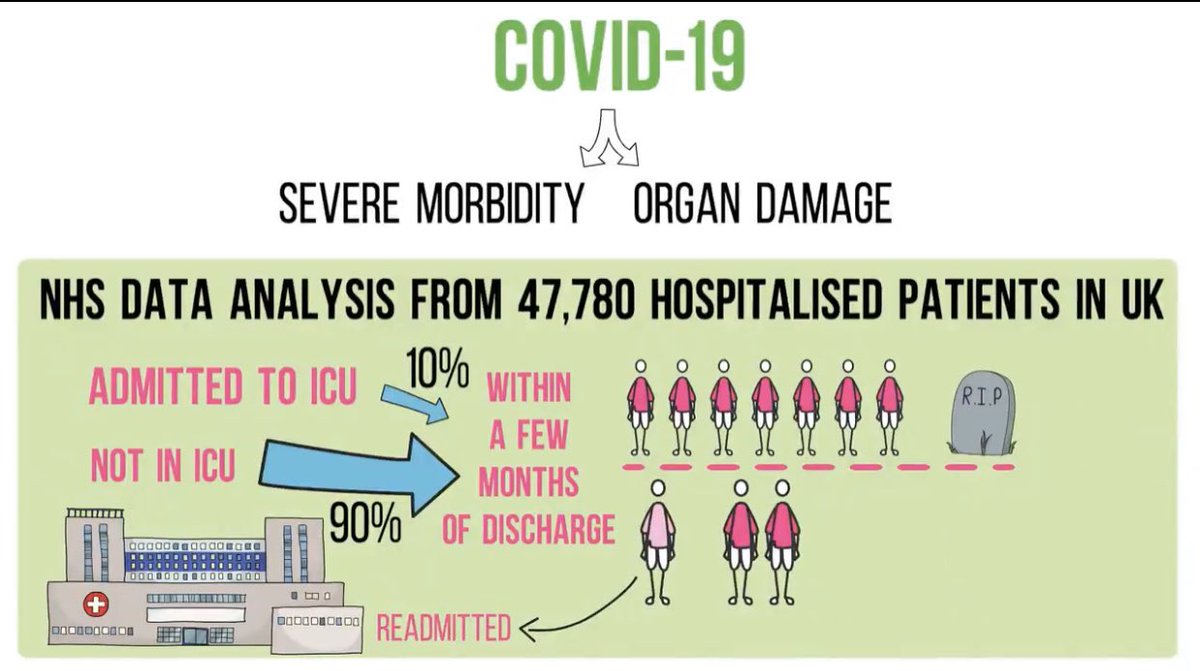
Wow. 1 in 3 hospitalized with #COVID19 gets readmitted to the hospital within a few months after discharge. ~48,000 UK patients.
Great animated lecture on #LongCovid by @Dr2NisreenAlwan, animated by @VickiGSP using info from UK @IndependentSage experts.

2) Furthermore, 1 in 8 of those who were discharged subsequently die. And many suffer long term ailments like heart disease, liver, kidney, diabetes, and more. This doesn’t even include less clinical critical cognitive effects. #LongCovid is real.
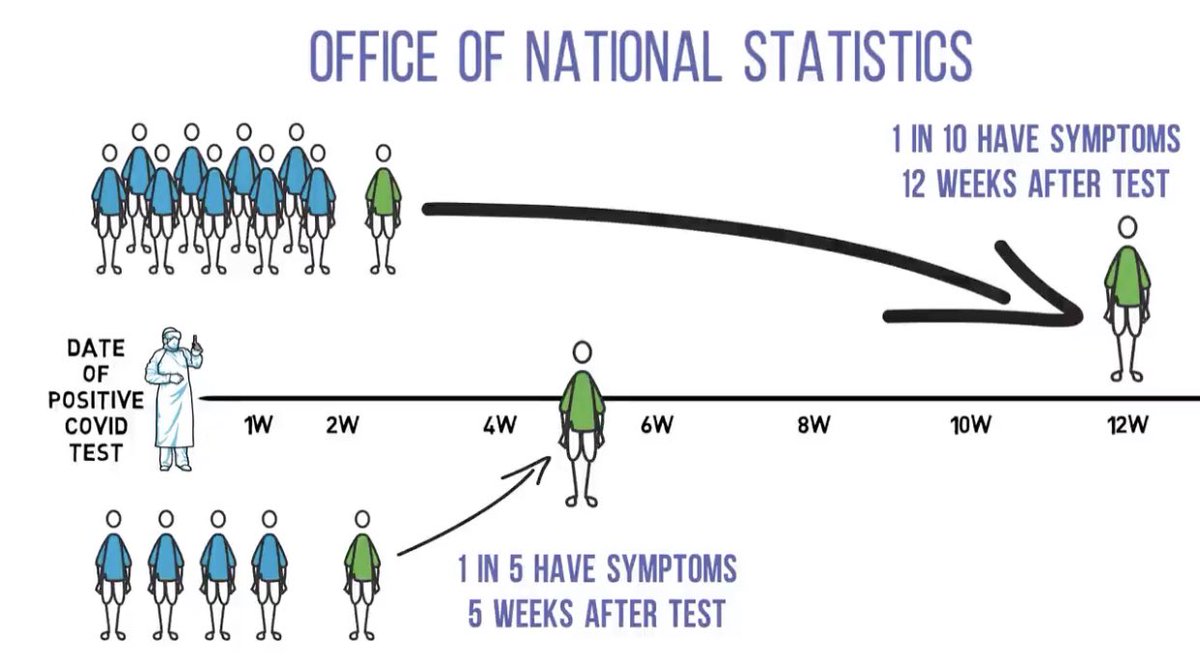
3) How common is #LongCovid overall? UK estimates 1 in 5 at 5 weeks and 1 in 10 have symptoms have even 12 weeks after initial #COVID19 diagnosis.
Lecture again by @Dr2NisreenAlwan

4) Let these numbers sink in... 1 in 10 at 12 weeks still have symptoms!
5) Here is the original study of the above lecture from few weeks ago. We need to prepare our healthcare system long term for the impact of millions with #LongCovid. This is gonna be larger than Gulf War Syndrome or long term health of 9/11 first responders.
Great animated lecture on #LongCovid by @Dr2NisreenAlwan, animated by @VickiGSP using info from UK @IndependentSage experts.
2) Furthermore, 1 in 8 of those who were discharged subsequently die. And many suffer long term ailments like heart disease, liver, kidney, diabetes, and more. This doesn’t even include less clinical critical cognitive effects. #LongCovid is real.
3) How common is #LongCovid overall? UK estimates 1 in 5 at 5 weeks and 1 in 10 have symptoms have even 12 weeks after initial #COVID19 diagnosis.
Lecture again by @Dr2NisreenAlwan
4) Let these numbers sink in... 1 in 10 at 12 weeks still have symptoms!
5) Here is the original study of the above lecture from few weeks ago. We need to prepare our healthcare system long term for the impact of millions with #LongCovid. This is gonna be larger than Gulf War Syndrome or long term health of 9/11 first responders.
LONG COVID\u201430% of hospital recovered #COVID19 patients end up back in hospital in <5 months; up to 12% die of complications. \u201cwe really need to prepare for #LongCovid. It\u2019s a mammoth task to follow up w/ these patients, but monitoring needs to be arranged\u201dhttps://t.co/h0y8WUn8sQ pic.twitter.com/Pk8GhQc9J5
— Eric Feigl-Ding (@DrEricDing) January 18, 2021
JUST ONE PERSON—UK 🇬🇧 scientists think one immunocompromised person who cleared virus slowly & only partially wiped out an infection, leaving behind genetically-hardier viruses that rebound & learn how to survive better. That’s likely how #B117 started. 🧵 https://t.co/bMMjM8Hiuz
2) The leading hypothesis is that the new variant evolved within just one person, chronically infected with the virus for so long it was able to evolve into a new, more infectious form.
same thing happened in Boston in another immunocompromised person that was sick for 155 days.
3) What happened in Boston with one 45 year old man who was highly infectious for 155 days straight before he died... is exactly what scientists think happened in Kent, England that gave rise to #B117.
4) Doctors were shocked to find virus has evolved many different forms inside of this one immunocompromised man. 20 new mutations in one virus, akin to the #B117. This is possibly how #B1351 in South Africa 🇿🇦 and #P1 in Brazil 🇧🇷 also evolved.
5) “On its own, the appearance of a new variant in genomic databases doesn’t tell us much. “That’s just one genome amongst thousands every week. It wouldn’t necessarily stick out,” says Oliver Pybus, a professor of evolution and infectious disease at Oxford.
2) The leading hypothesis is that the new variant evolved within just one person, chronically infected with the virus for so long it was able to evolve into a new, more infectious form.
same thing happened in Boston in another immunocompromised person that was sick for 155 days.
3) What happened in Boston with one 45 year old man who was highly infectious for 155 days straight before he died... is exactly what scientists think happened in Kent, England that gave rise to #B117.
Immunocompromised 45 year old suffered from #COVID19 for 155 days before he died. The virus was changing very quickly inside the man's body\u2014it acquired a big cluster of >20 mutations\u2014resembled the same ones seen in #B117 & #B1351. (NPR audio Part 1 of 2)\U0001f9f5https://t.co/7kWiBZ1xGk pic.twitter.com/ZJ7AExB78Y
— Eric Feigl-Ding (@DrEricDing) February 8, 2021
4) Doctors were shocked to find virus has evolved many different forms inside of this one immunocompromised man. 20 new mutations in one virus, akin to the #B117. This is possibly how #B1351 in South Africa 🇿🇦 and #P1 in Brazil 🇧🇷 also evolved.
2) NPR report audio part 2 of 2:
— Eric Feigl-Ding (@DrEricDing) February 8, 2021
Dr. Li couldn't believe what they found. "I was shocked," he says. "When I saw the virus sequences, I knew that we were dealing with something completely different and potentially very important." pic.twitter.com/HT3Yt6djFd
5) “On its own, the appearance of a new variant in genomic databases doesn’t tell us much. “That’s just one genome amongst thousands every week. It wouldn’t necessarily stick out,” says Oliver Pybus, a professor of evolution and infectious disease at Oxford.
Breaking—UK scientists just reported a case-control study that the mutated UK 🇬🇧B.1.1.7 variant is not associated w/ more severe #COVID19— “found no significant differences in hospital admissions and case fatality at 28 days, & occurrence of reinfections”, says @mvankerkhove
2) That said, the new UK mutated strain is a more transmissible (contagious) variant. Keep transmissibility and illness severity separate. They are two different things. Don’t get them confused.
3) The new UK variant severity study is included in today’s WHO report, to be released soon this afternoon according to WHO sources. Waiting for it to drop. I’ll keep folks posted on the details.
4) Update: here is UK Technical report on #SARSCoV2 variant of concern (B.1.1.7) in 🇬🇧 with prelim findings from their case-control study of no increased severity for the new variant that I reported yesterday.
5) Also keep in a mind that a virus that spreads faster (more contagious) yields much worse total outcomes than a virus that is just merely more severe.
All things equal, a new mutated variant that is more contagious & no more severe is worse. And that is what we now have.
2) That said, the new UK mutated strain is a more transmissible (contagious) variant. Keep transmissibility and illness severity separate. They are two different things. Don’t get them confused.
3) The new UK variant severity study is included in today’s WHO report, to be released soon this afternoon according to WHO sources. Waiting for it to drop. I’ll keep folks posted on the details.
4) Update: here is UK Technical report on #SARSCoV2 variant of concern (B.1.1.7) in 🇬🇧 with prelim findings from their case-control study of no increased severity for the new variant that I reported yesterday.
5) Also keep in a mind that a virus that spreads faster (more contagious) yields much worse total outcomes than a virus that is just merely more severe.
All things equal, a new mutated variant that is more contagious & no more severe is worse. And that is what we now have.
Why a SARS-CoV-2 variant that's 50% more transmissible would in general be a much bigger problem than a variant that's 50% more deadly. A short thread... 1/
— Adam Kucharski (@AdamJKucharski) December 28, 2020
JUST IN — "Camp Auschwitz" insurrectionist of the Capitol siege was just arrested this morning in Newport News, VIrginia.
2) this guy was just arrested.

3) We cannot have a repeat of the fascism from WW2. This is @Schwarzenegger’s speech was so powerful.
4) My wife @andreafeigl1’s 🇦🇹 great grandfather secretly fought Hilter’s Nazi regime & smuggled many Jews to safety as an aircraft engineer. He was thrown into a concentration camp, and escaped.
She knows a few things about Nazi history—Jan 6th was downright fascist. Read 👇
5) So this cover is from a semi-tabloid magazine in Germany, according to @andreafeigl1. But even so, how did such a magazine still get it so damn right?! Maybe Germany 🇩🇪 has seen this kinda fascism before...

2) this guy was just arrested.
3) We cannot have a repeat of the fascism from WW2. This is @Schwarzenegger’s speech was so powerful.
This speech will go down as one of the greatest speeches. @Schwarzenegger is right\u2014Jan 6th 2021 was our Kristallnacht. Austria \U0001f1e6\U0001f1f9 tried to resist Hilter takeover for years but succumbed because Hitler\u2019s lies went unchallenged. We must #impeach now. pic.twitter.com/gOChiGLuHK
— Eric Feigl-Ding (@DrEricDing) January 10, 2021
4) My wife @andreafeigl1’s 🇦🇹 great grandfather secretly fought Hilter’s Nazi regime & smuggled many Jews to safety as an aircraft engineer. He was thrown into a concentration camp, and escaped.
She knows a few things about Nazi history—Jan 6th was downright fascist. Read 👇
Some saw clearly what MAGAism is - pure fascism - in 2016.
— Dr. Andrea Feigl (@andreafeigl1) January 6, 2021
More see it 2day
Some saw this playbook b4: WW2
Americans r too unaware of history since it didn't happen on home soil
But we MUST heed these lessons, lest it b 2 late 4 democracy & consequences are unfathomable
\U0001f9f5 pic.twitter.com/QdoVG3LsrB
5) So this cover is from a semi-tabloid magazine in Germany, according to @andreafeigl1. But even so, how did such a magazine still get it so damn right?! Maybe Germany 🇩🇪 has seen this kinda fascism before...
More from Health

1/16
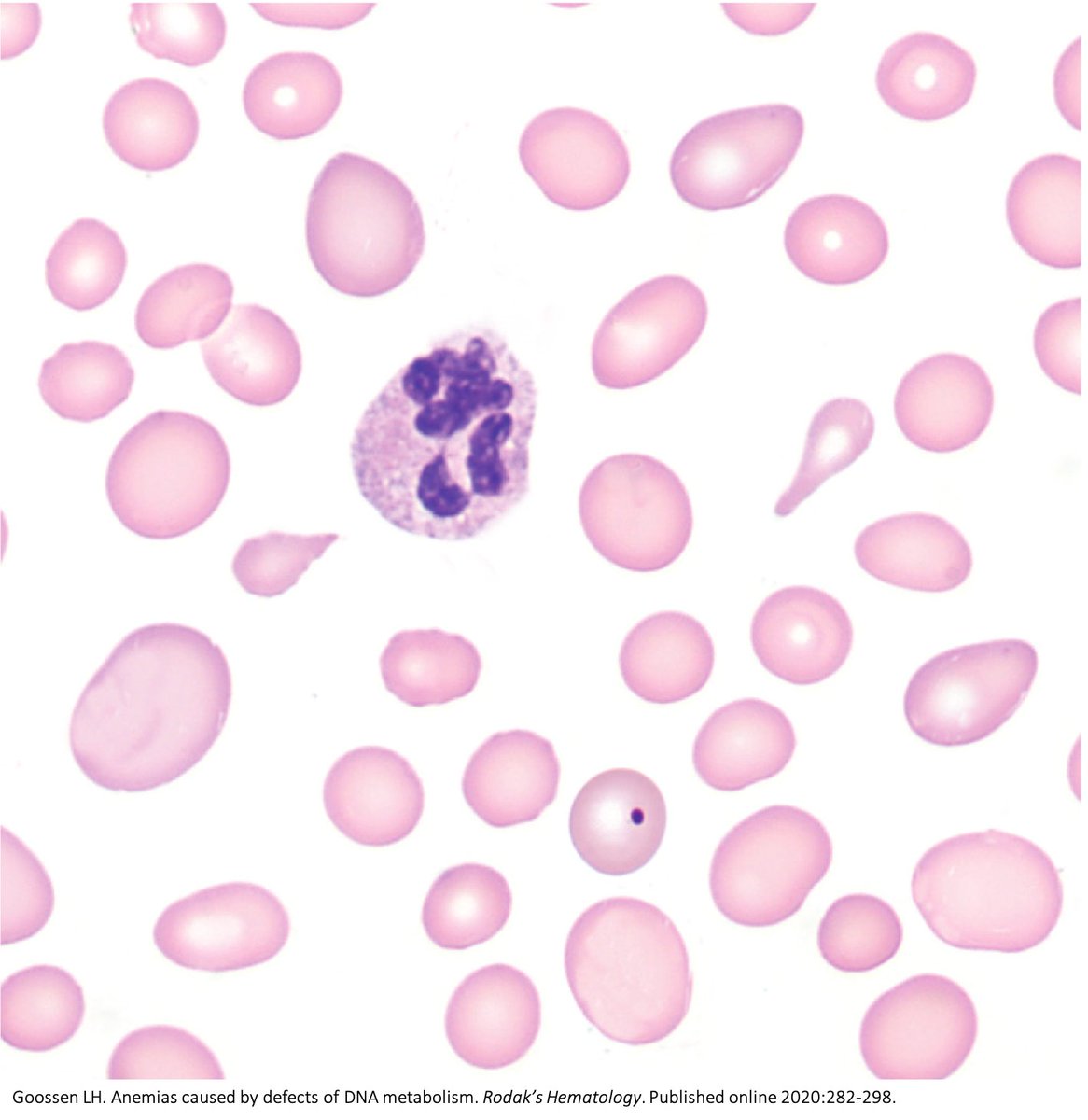
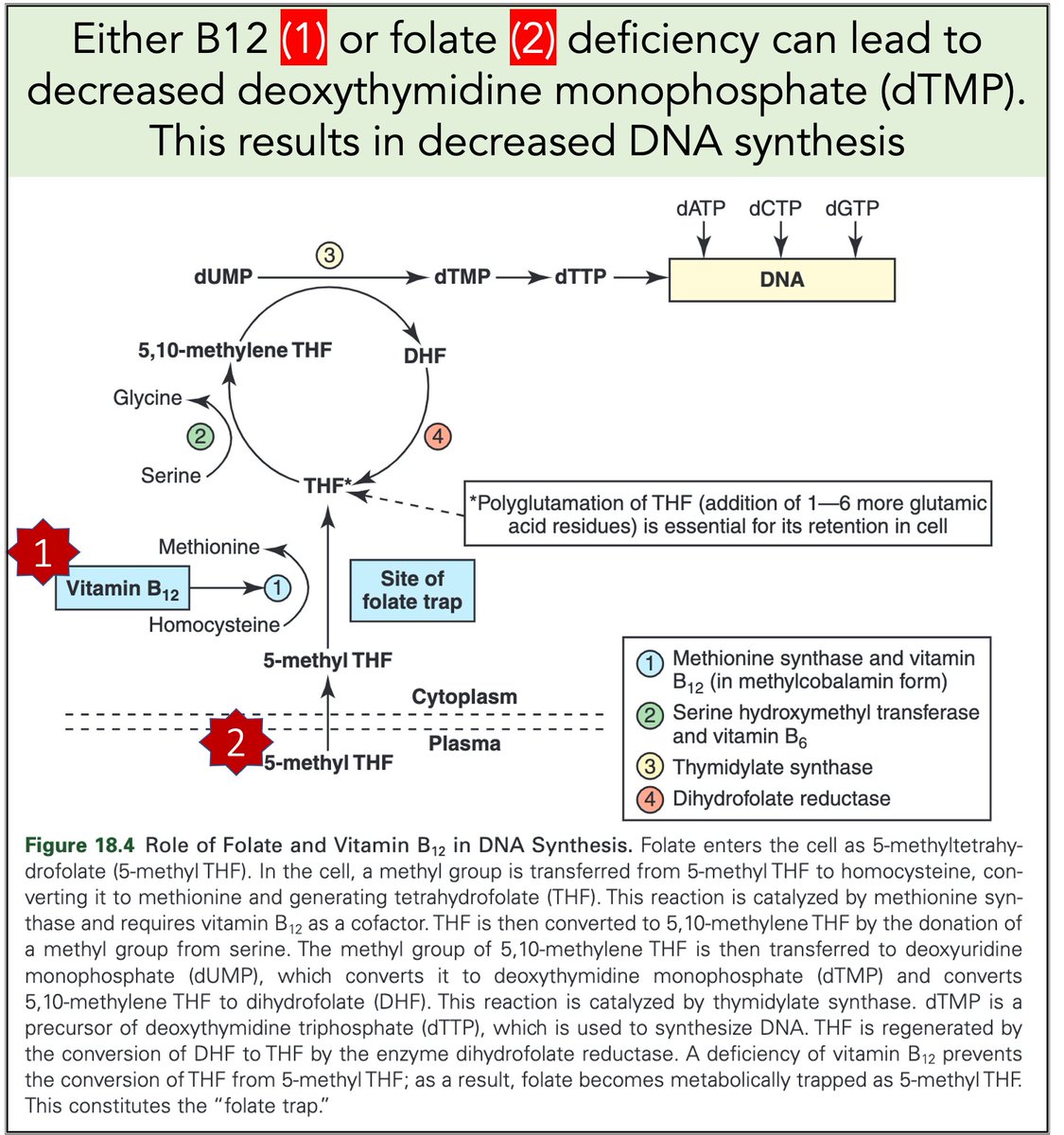
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
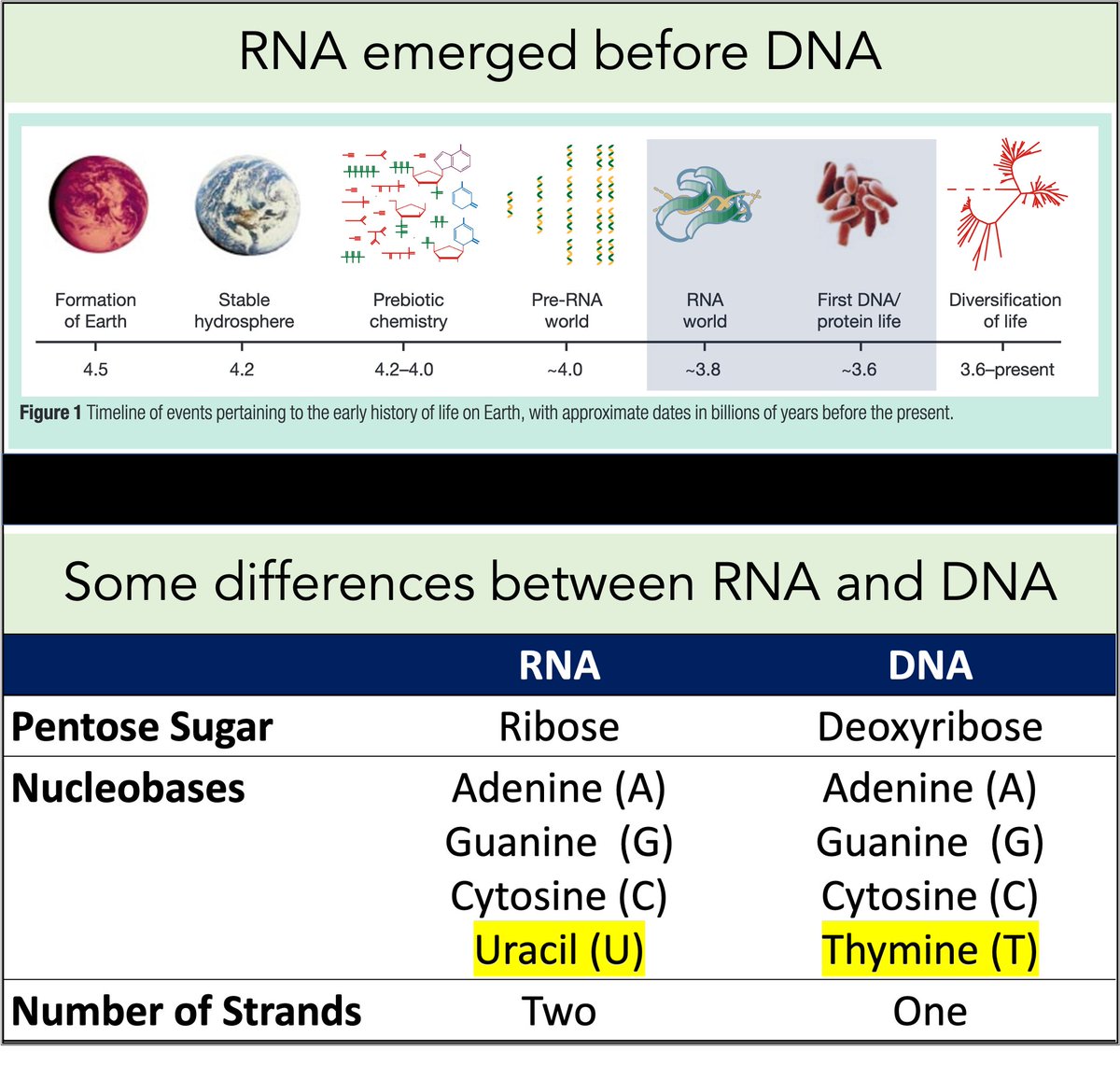
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
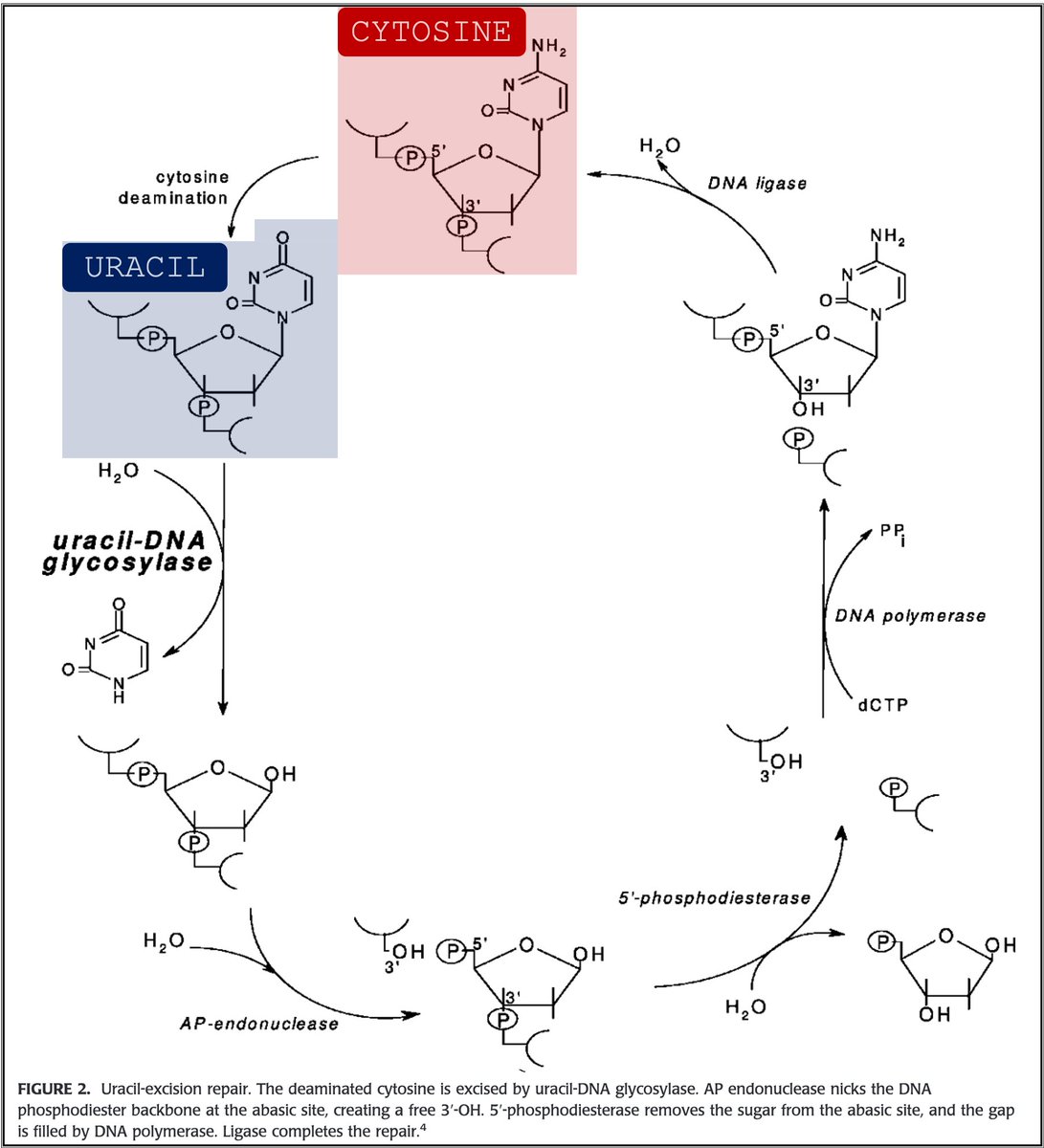
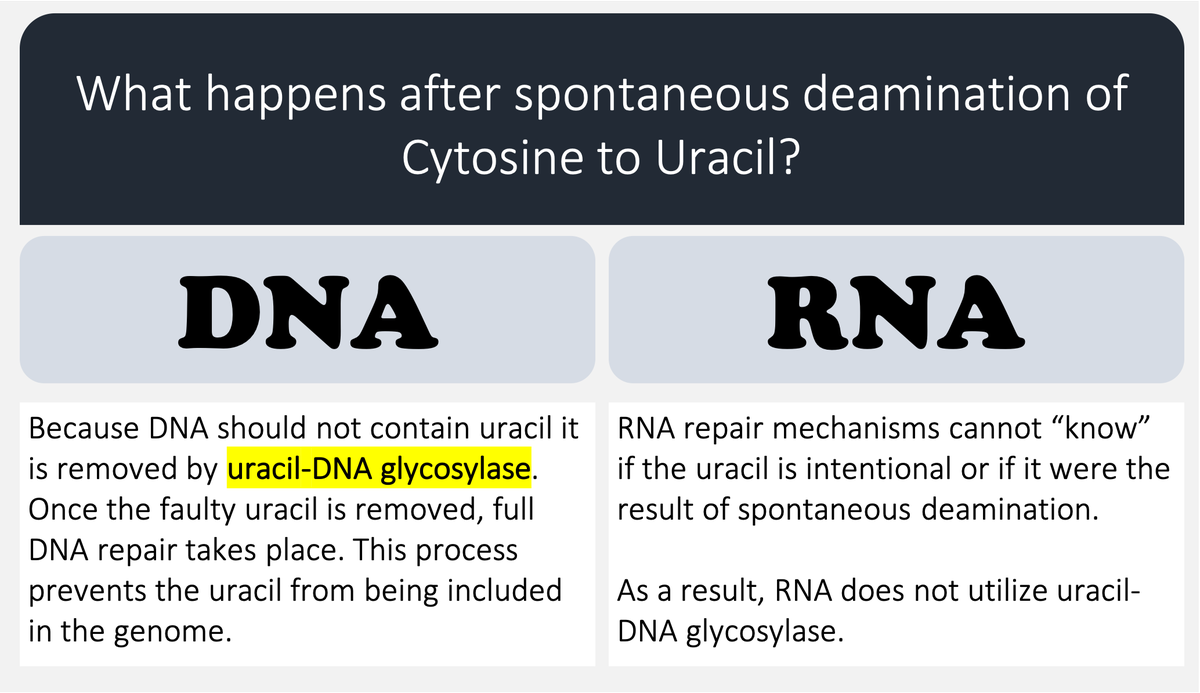
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh


🚨New lockdown regulations just published, in force tomorrow
The Health Protection (Coronavirus, Restrictions) (No. 3) and (All Tiers) (England) (Amendment) Regulations 2021
https://t.co/L5jwlTDaIE
(Thread)
These are not a new set of regulations: they are amendments an old set of regulations
Which we thought were gone! But they are back
Welcome back No.3 regulations
A quick thing before we continue!
I have been analysing these laws for free for 9 months now - if you want to say thanks and have a few £ to spare please give to my @LawCentres fundraiser
They give free legal advice to people who need it
They also amend the All Tiers regulations
Oh god it's all amendments by paragraph references
Basically all of England now in Tier 4 and Tier 4 is amended but not by a huge amount
This really is a terrible way to make laws on the fly - who can possibly understand it?!
So, to explain, you need 2 documents open if you want to understand what is going on:
All Tiers regulations (Tiers 1-4, 2 December as amended) https://t.co/IraPQ112ak
And amendments https://t.co/L5jwlTDaIE
No sensible way of doing except by track changes, on it now, back soon
The Health Protection (Coronavirus, Restrictions) (No. 3) and (All Tiers) (England) (Amendment) Regulations 2021
https://t.co/L5jwlTDaIE
(Thread)
These are not a new set of regulations: they are amendments an old set of regulations
Which we thought were gone! But they are back
Welcome back No.3 regulations
A quick thing before we continue!
I have been analysing these laws for free for 9 months now - if you want to say thanks and have a few £ to spare please give to my @LawCentres fundraiser
They give free legal advice to people who need it
They also amend the All Tiers regulations
Oh god it's all amendments by paragraph references
Basically all of England now in Tier 4 and Tier 4 is amended but not by a huge amount
This really is a terrible way to make laws on the fly - who can possibly understand it?!
So, to explain, you need 2 documents open if you want to understand what is going on:
All Tiers regulations (Tiers 1-4, 2 December as amended) https://t.co/IraPQ112ak
And amendments https://t.co/L5jwlTDaIE
No sensible way of doing except by track changes, on it now, back soon