
There is *real* anger toward this organization. Honestly, more than I even heard about from MD students and the NBME.
You asked. So here are my thoughts on how osteopathic medical students should respond to the NBOME.
(thread)
I think most of us are over here waiting to see what @jbcarmody has to say about the latest NBOME email pic.twitter.com/bVWkS23V7z
— Jake Berg (@jberg521) January 28, 2021
There is *real* anger toward this organization. Honestly, more than I even heard about from MD students and the NBME.
Amorphous anger on social media is easy to ignore. But if that anger gets channeled into organized efforts to facilitate change, then improvements are possible.
Best case scenario, you’ll get another “town hall” meeting, a handful of platitudes, and some thoughtful beard stroking before being told that they’re keeping the exam.
Almost all states allow DO licensure by completing the USMLE series. If you aren’t required to engage with the NBOME, don’t.
As an MD who has passed the USMLE, I could practice in any state. Why shouldn’t a DO who passed the USMLE be able to do the same?
(State boards that prop up the NBOME with a COMLEX requirement are listed in the Tweet below.) https://t.co/stace4lMjD
For those wondering, DO students who completed Step1 & Step2CK are eligible to sit for Step3 and receive state licensure w/o COMLEX series in ~44/50 states; 5 states can accommodate others w/o Level2PE; 1 state, FL, does not.
— Mustafa Basree MS (@mustafabasree) January 26, 2021
See below if you're considering below 5 states \U0001f447\U0001f3fd
The board may be friendly with the NBOME, but they’re still accountable to the legislature.
It’s ultimately the COCA requirement that keeps the NBOME in business.
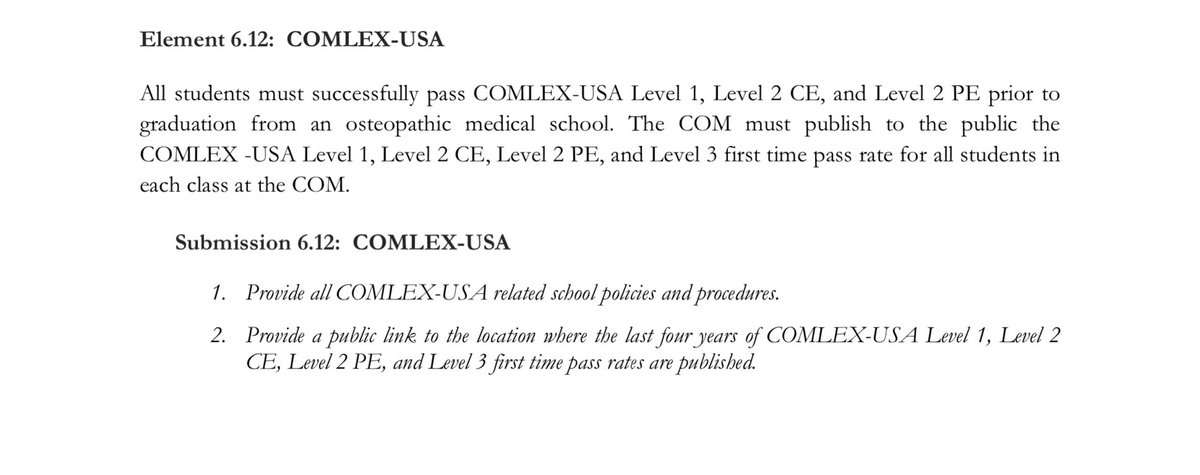
They should think carefully about whether, at this point in history, a “separate but equal” licensing exam hurts DOs more than it helps.
https://t.co/pFwaAx01oB

More from Education


Trending news of The Rock's daughter Simone Johnson's announcing her new Stage Name is breaking our Versus tool because "Wrestling Name" isn't in our database!
Here's the most useful #Factualist comparison pages #Thread 🧵

What is the difference between “pseudonym” and “stage name?”
Pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie stars,” while stage name is “the pseudonym of an entertainer.”
https://t.co/hT5XPkTepy #english #wiki #wikidiff
People also found this comparison helpful:
Alias #versus Stage Name: What’s the difference?
Alias means “another name; an assumed name,” while stage name means “the pseudonym of an entertainer.”
https://t.co/Kf7uVKekMd #Etymology #words
Another common #question:
What is the difference between “alias” and “pseudonym?”
As nouns alias means “another name; an assumed name,” while pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie
Here is a very basic #comparison: "Name versus Stage Name"
As #nouns, the difference is that name means “any nounal word or phrase which indicates a particular person, place, class, or thing,” but stage name means “the pseudonym of an
Here's the most useful #Factualist comparison pages #Thread 🧵
What is the difference between “pseudonym” and “stage name?”
Pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie stars,” while stage name is “the pseudonym of an entertainer.”
https://t.co/hT5XPkTepy #english #wiki #wikidiff
People also found this comparison helpful:
Alias #versus Stage Name: What’s the difference?
Alias means “another name; an assumed name,” while stage name means “the pseudonym of an entertainer.”
https://t.co/Kf7uVKekMd #Etymology #words
Another common #question:
What is the difference between “alias” and “pseudonym?”
As nouns alias means “another name; an assumed name,” while pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie
Here is a very basic #comparison: "Name versus Stage Name"
As #nouns, the difference is that name means “any nounal word or phrase which indicates a particular person, place, class, or thing,” but stage name means “the pseudonym of an

A list of cool websites you might now know about
A thread 🧵
1) Learn Anything - Search tools for knowledge discovery that helps you understand any topic through the most efficient
2) Grad Speeches - Discover the best commencement speeches.
This website is made by me
3) What does the Internet Think - Find out what the internet thinks about anything
4) https://t.co/vuhT6jVItx - Send notes that will self-destruct after being read.
A thread 🧵
1) Learn Anything - Search tools for knowledge discovery that helps you understand any topic through the most efficient
2) Grad Speeches - Discover the best commencement speeches.
This website is made by me
3) What does the Internet Think - Find out what the internet thinks about anything
4) https://t.co/vuhT6jVItx - Send notes that will self-destruct after being read.


You May Also Like

















A list of cool websites you might now know about
A thread 🧵
1) Learn Anything - Search tools for knowledge discovery that helps you understand any topic through the most efficient
2) Grad Speeches - Discover the best commencement speeches.
This website is made by me
3) What does the Internet Think - Find out what the internet thinks about anything
4) https://t.co/vuhT6jVItx - Send notes that will self-destruct after being read.
A thread 🧵
1) Learn Anything - Search tools for knowledge discovery that helps you understand any topic through the most efficient
2) Grad Speeches - Discover the best commencement speeches.
This website is made by me
3) What does the Internet Think - Find out what the internet thinks about anything
4) https://t.co/vuhT6jVItx - Send notes that will self-destruct after being read.