Thread on the recent report on the possible risk of increased death associated with the new UK variant (B117)- with a discussion of the evidence around this, and what this means.
Increased fatality rates also increase deaths- but do so linearly.
https://t.co/nqV3udZByu
How dangerous are the B.1.1.7 and 501Y.V2 hyper-transmissible strains?
— Eric Topol (@EricTopol) January 11, 2021
by @AdamJKucharski @CFR_orghttps://t.co/aycWMN3b5h
h/t @Karl_Lauterbach pic.twitter.com/JlaFzzP06t
We don't routinely sequence all samples for the virus. We've found that the variant has a particular deletion which means that some PCR tests on samples with the variant give a different read-out when the variant is present.
Different analyses carried out with the data in slightly different ways suggested a ~1.3x increase in risk of death.
Unlikely. The people with the B117 variant were matched to controls by age, specimen data, and location - so they would've been compared with people infected at the same time, in the same area.
Possibly. A theoretical reason is that people who are infected with the new more transmissible variant are different in some other way- that makes them more likely to die anyway were they infected with any variant.
To me, this highlights the gambles we take when we follow an approach which allows high levels of transmission to continue in the community for long periods of time. The UK govt has consistently minimised the risk posed by COVID-19, which is why we're here.
Hoping for the best, and dealing with variants after they get out of hand doesn't work. We need to proactively contain these.
Australia imported the UK variant, but they acted aggressively to prevent it establishing in the community
More from Deepti Gurdasani
This is the exact problem with our government's thinking & response- despite this strategy of 'tolerating deaths' and half-way measures having spectacularly failed, it's quite amazing that our govt still hasn't learned anything, & continues to promote a policy of death. Thread
Had we adopted an elimination strategy early on, rather than one of tolerating a certain level of infection, we wouldn't be here now. The reason we're here is because the govt never committed to elimination.
We eased lockdown in May when infection levels were much higher than when other countries in Europe did this. The govt was warned about this, but did this to 'help the economy'. Not only did this lead us into the 2nd wave, the need for further lockdowns harmed the economy further
It's very clear from global evidence that we cannot 'tolerate a level of community transmission' and maintain 'R at or just below 1', which has been our governments policy for a long time. This isn't sustainable & very rapidly gets out of control, leading to exponential rises
Coupled with late action to contain these surges, not only does this lead to many more deaths, and much more morbidity with Long COVID, it also creates a fertile ground for viral mutations to accumulate with a greater risk of adaptation, which is exactly what happened in the UK
U.K. needs to confront
— Esther McVey (@EstherMcVey1) January 2, 2021
\u2018The challenge that faces us is to decide - are we going to try to pursue the elimination of Covid-19 regardless of the costs or decide on a tolerable level of deaths (like we do with the flu) in order to return to a normal life?\u2019
https://t.co/9hWbHIPJUq
Had we adopted an elimination strategy early on, rather than one of tolerating a certain level of infection, we wouldn't be here now. The reason we're here is because the govt never committed to elimination.
We eased lockdown in May when infection levels were much higher than when other countries in Europe did this. The govt was warned about this, but did this to 'help the economy'. Not only did this lead us into the 2nd wave, the need for further lockdowns harmed the economy further
It's very clear from global evidence that we cannot 'tolerate a level of community transmission' and maintain 'R at or just below 1', which has been our governments policy for a long time. This isn't sustainable & very rapidly gets out of control, leading to exponential rises
Coupled with late action to contain these surges, not only does this lead to many more deaths, and much more morbidity with Long COVID, it also creates a fertile ground for viral mutations to accumulate with a greater risk of adaptation, which is exactly what happened in the UK
Brief thread to debunk the repeated claims we hear about transmission not happening 'within school walls', infection in school children being 'a reflection of infection from the community', and 'primary school children less likely to get infected and contribute to transmission'.
I've heard a lot of scientists claim these three - including most recently the chief advisor to the CDC, where the claim that most transmission doesn't happen within the walls of schools. There is strong evidence to rebut this claim. Let's look at
Let's look at the trends of infection in different age groups in England first- as reported by the ONS. Being a random survey of infection in the community, this doesn't suffer from the biases of symptom-based testing, particularly important in children who are often asymptomatic
A few things to note:
1. The infection rates among primary & secondary school children closely follow school openings, closures & levels of attendance. E.g. We see a dip in infections following Oct half-term, followed by a rise after school reopening.
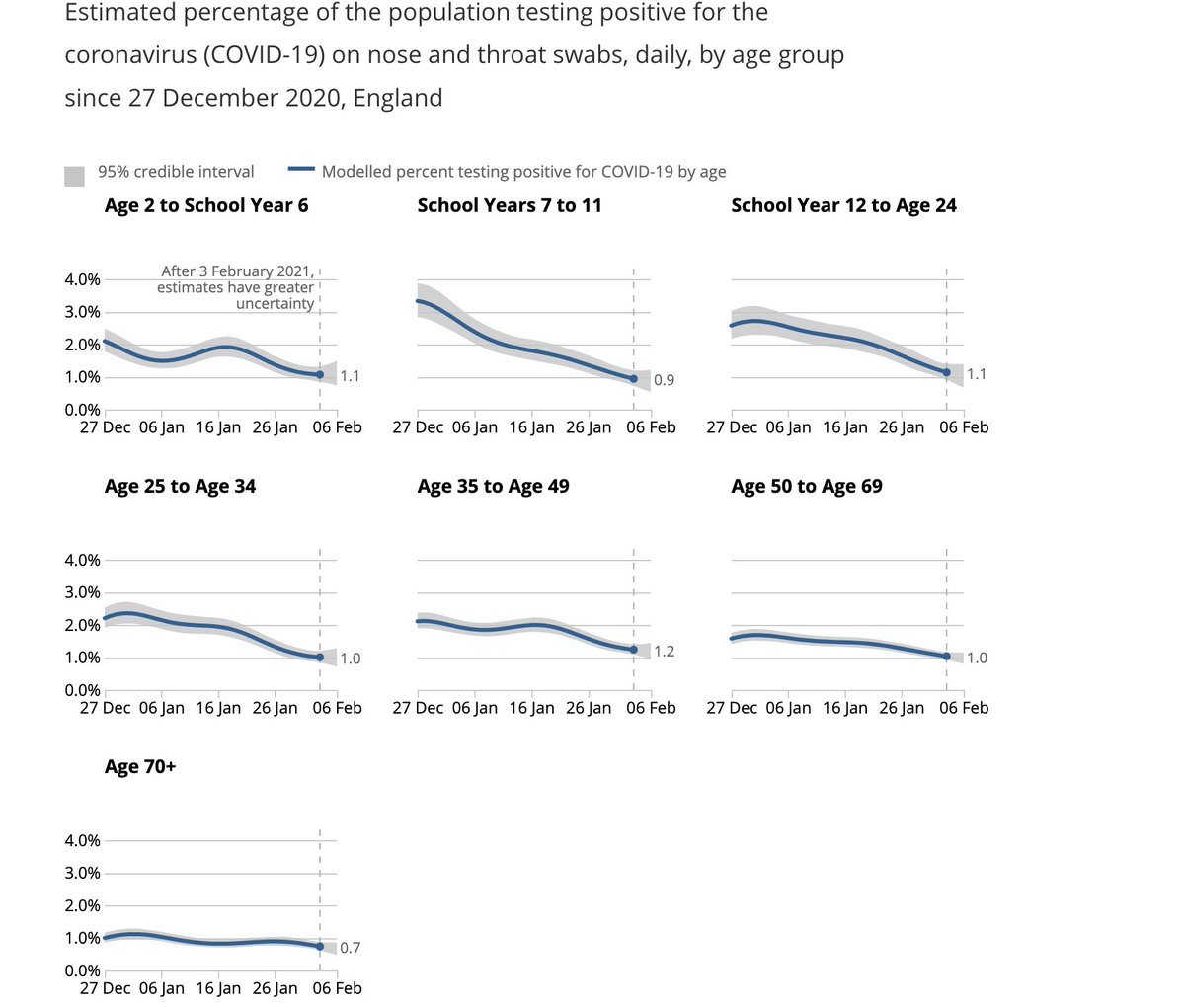
We see steep drops in both primary & secondary school groups after end of term (18th December), but these drops plateau out in primary school children, where attendance has been >20% after re-opening in January (by contrast with 2ndary schools where this is ~5%).
I've heard a lot of scientists claim these three - including most recently the chief advisor to the CDC, where the claim that most transmission doesn't happen within the walls of schools. There is strong evidence to rebut this claim. Let's look at
The science shows us that most disease transmission does not happen in the walls of the school, but it comes in from the community. So, CDC is advocating to get our K-5 students back in school at least in a hybrid mode with universal mask wearing and 6 ft of distancing. https://t.co/dfvJ2nl2s4
— Rochelle Walensky, MD, MPH (@CDCDirector) February 14, 2021
Let's look at the trends of infection in different age groups in England first- as reported by the ONS. Being a random survey of infection in the community, this doesn't suffer from the biases of symptom-based testing, particularly important in children who are often asymptomatic
A few things to note:
1. The infection rates among primary & secondary school children closely follow school openings, closures & levels of attendance. E.g. We see a dip in infections following Oct half-term, followed by a rise after school reopening.
We see steep drops in both primary & secondary school groups after end of term (18th December), but these drops plateau out in primary school children, where attendance has been >20% after re-opening in January (by contrast with 2ndary schools where this is ~5%).
We've been falsely told 'schools are safe', 'don't drive community transmission', & teachers don't have a higher risk of infection repeatedly by govt & their advisors- to justify some of the most negligent policies in history. 🧵
data shows *both* primary & secondary school teachers are at double the risk of confirmed infection relative to comparable positivity in the general population. ONS household infection data also clearly show that children are important sources of transmission.
Yet, in the parliamentary select meeting today, witnesses like Jenny Harries repeated the same claims- that have been debunked by the ONS data, and the data released by the @educationgovuk today. How many lives have been lost to these lies? How many more people have long COVID?
has repeatedly pointed out errors & gaps in the ONS reporting of evidence around risk of infection among teachers- and it's taken *months* to get clarity on this. The released data are a result of months of campaigning by her, the @NEU and others.
Rather than being transparent about the risk of transmission in school settings & mitigating this, the govt (& many of its advisors) has engaged in dismissing & denying evidence that's been clear for a while. Evidence from the govt's own surveys. And global evidence.
Why?
Questions have to be asked about the evidence Jenny Harries gave to the Education Committee today about the risk to teachers.
— Adam Hamdy (@adamhamdy) January 19, 2021
Was she aware of this data?
If not, why wasn\u2019t she properly briefed?#COVID19 #schools https://t.co/4wa1PyAJld pic.twitter.com/eqFjaA1zYC
data shows *both* primary & secondary school teachers are at double the risk of confirmed infection relative to comparable positivity in the general population. ONS household infection data also clearly show that children are important sources of transmission.
Yet, in the parliamentary select meeting today, witnesses like Jenny Harries repeated the same claims- that have been debunked by the ONS data, and the data released by the @educationgovuk today. How many lives have been lost to these lies? How many more people have long COVID?
has repeatedly pointed out errors & gaps in the ONS reporting of evidence around risk of infection among teachers- and it's taken *months* to get clarity on this. The released data are a result of months of campaigning by her, the @NEU and others.
Rather than being transparent about the risk of transmission in school settings & mitigating this, the govt (& many of its advisors) has engaged in dismissing & denying evidence that's been clear for a while. Evidence from the govt's own surveys. And global evidence.
Why?