
The idea is planted in people’s mind that this virus is mutating in such a way as to evade prior immunity. This is completely unfounded, certainly as regards immunity..
In a number of Sunday papers:
Scientific advisers said it was “hard to see” when the restrictions would end as new variants continued to emerge, delivering a potentially devastating blow to the travel industry. The prime minister said that after progress with vaccinations...
The idea is planted in people’s mind that this virus is mutating in such a way as to evade prior immunity. This is completely unfounded, certainly as regards immunity..
To mutations & variants. Many viruses are error-prone when they replicate in your cells. They make “typos” so the virus which results is...
Why these incorrect stories are being spun, I’ve no idea, that not being a scientific matter. But spin & completely inappropriate & severe restrictions...
More from Yardley Yeadon



I urge all followers who have read my criticisms of PCR mass testing in U.K. to carefully read Mr Fordham’s carefully worded letter. Note that the innovation minister in the Lords, Lord Bethel, already admitted that the PCR system doesn’t have the equivalent of an MOT. https://t.co/zXzeDMKCBb

Without this information it’s impossible to interpret any result. If the oFPR is 4%, for example, and if the true prevalence is 0.3% (it’s probably less), then for every 10,000 tests, 400 positives would be false & 30 positives would be genuine. So 93% of positives are false.
As Mr Fordham points out, almost all policies pivot on PCR mass testing. Hancock previously admitted on talkRADIO to Julia Hartley-Brewer in late summer that the FPR was “just under 1%”. That was a flat lie (possibly inadvertent but he’s never corrected the record). The reason...
...we are sure Hancock told a lie is that they have never known the FPR. Those including Hancock who believe that the oFPR can be estimated by inspection of the lowest positivity ever recorded, while logical, is completely wrong. Changes in personnel, throughout, testing...
...architecture & the like can radically alter the oFPR. Since Hancock’s remark in late summer, PCR mass testing has moved into the Lighthouse Labs & this creates a new & urgent need to continually assess oFPR. I’ve good reason to believe it’s now VERY much higher now that the...
So I wrote back to @lucyfrazermp for another go. Here\u2019s my letter.
— Edmund Fordham (@EdmundFordham) November 28, 2020
They don\u2019t understand how serious this is.
If they can\u2019t tell us the oFPR, our PCR testing is worthless. (thread) pic.twitter.com/zHJ8SJCzf1
Without this information it’s impossible to interpret any result. If the oFPR is 4%, for example, and if the true prevalence is 0.3% (it’s probably less), then for every 10,000 tests, 400 positives would be false & 30 positives would be genuine. So 93% of positives are false.
As Mr Fordham points out, almost all policies pivot on PCR mass testing. Hancock previously admitted on talkRADIO to Julia Hartley-Brewer in late summer that the FPR was “just under 1%”. That was a flat lie (possibly inadvertent but he’s never corrected the record). The reason...
...we are sure Hancock told a lie is that they have never known the FPR. Those including Hancock who believe that the oFPR can be estimated by inspection of the lowest positivity ever recorded, while logical, is completely wrong. Changes in personnel, throughout, testing...
...architecture & the like can radically alter the oFPR. Since Hancock’s remark in late summer, PCR mass testing has moved into the Lighthouse Labs & this creates a new & urgent need to continually assess oFPR. I’ve good reason to believe it’s now VERY much higher now that the...


More from Science









You May Also Like

First update to https://t.co/lDdqjtKTZL since the challenge ended – Medium links!! Go add your Medium profile now 👀📝 (thanks @diannamallen for the suggestion 😁)

Just added Telegram links to https://t.co/lDdqjtKTZL too! Now you can provide a nice easy way for people to message you :)

Less than 1 hour since I started adding stuff to https://t.co/lDdqjtKTZL again, and profile pages are now responsive!!! 🥳 Check it out -> https://t.co/fVkEL4fu0L
Accounts page is now also responsive!! 📱✨
💪 I managed to make the whole site responsive in about an hour. On my roadmap I had it down as 4-5 hours!!! 🤘🤠🤘
Just added Telegram links to https://t.co/lDdqjtKTZL too! Now you can provide a nice easy way for people to message you :)
Less than 1 hour since I started adding stuff to https://t.co/lDdqjtKTZL again, and profile pages are now responsive!!! 🥳 Check it out -> https://t.co/fVkEL4fu0L
Accounts page is now also responsive!! 📱✨
💪 I managed to make the whole site responsive in about an hour. On my roadmap I had it down as 4-5 hours!!! 🤘🤠🤘

So friends here is the thread on the recommended pathway for new entrants in the stock market.
Here I will share what I believe are essentials for anybody who is interested in stock markets and the resources to learn them, its from my experience and by no means exhaustive..
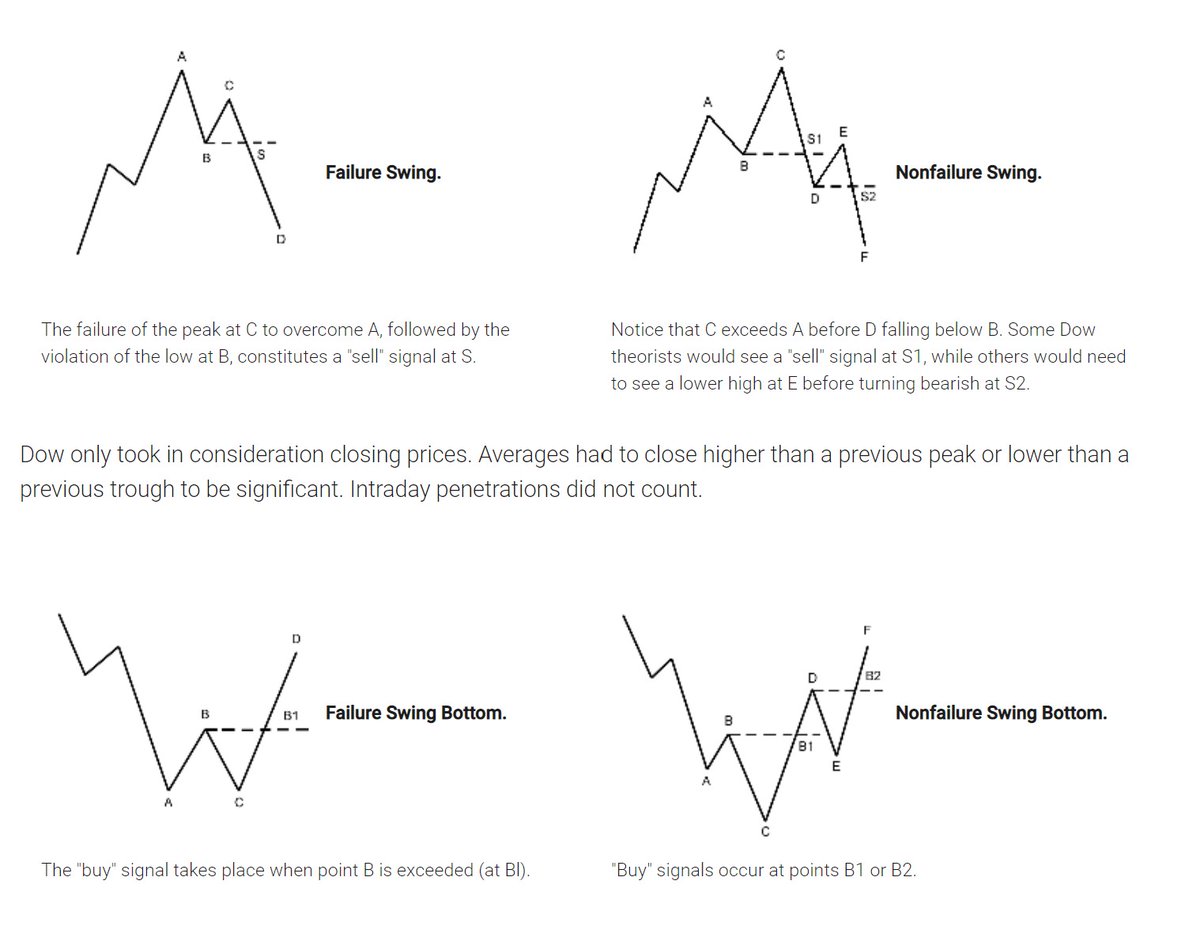
First the very basic : The Dow theory, Everybody must have basic understanding of it and must learn to observe High Highs, Higher Lows, Lower Highs and Lowers lows on charts and their
Even those who are more inclined towards fundamental side can also benefit from Dow theory, as it can hint start & end of Bull/Bear runs thereby indication entry and exits.
Next basic is Wyckoff's Theory. It tells how accumulation and distribution happens with regularity and how the market actually
Dow theory is old but
Here I will share what I believe are essentials for anybody who is interested in stock markets and the resources to learn them, its from my experience and by no means exhaustive..
First the very basic : The Dow theory, Everybody must have basic understanding of it and must learn to observe High Highs, Higher Lows, Lower Highs and Lowers lows on charts and their
Even those who are more inclined towards fundamental side can also benefit from Dow theory, as it can hint start & end of Bull/Bear runs thereby indication entry and exits.
Next basic is Wyckoff's Theory. It tells how accumulation and distribution happens with regularity and how the market actually
Dow theory is old but
Old is Gold....
— Professor (@DillikiBiili) January 23, 2020
this Bharti Airtel chart is a true copy of the Wyckoff Pattern propounded in 1931....... pic.twitter.com/tQ1PNebq7d

1/12
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
4/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
...indication, first of all that testing for a (single) respiratory virus is done outside of surveillance systems or need for specific therapy, but even so the lack of consideration of Ct, symptoms and clinical findings when interpreting its result. https://t.co/gHH6kwRdZG
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
6/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
The neither validated nor standardised hypersensitive RT-PCR test / Ct 35-45 for SARS-CoV-2 is abused to mislabel (also) other diseases, especially influenza, as COVID-19.https://t.co/AkFIfTCTkS
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.https://t.co/mbNY8bdw1p pic.twitter.com/OQBD4grMth
— Dr. Thomas Binder, MD (@Thomas_Binder) November 29, 2020
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
Thread web\u2b06\ufe0f\u2b07\ufe0f
— Dr. Thomas Binder, MD (@Thomas_Binder) December 16, 2020
The fabrication of the "asymptomatic (super) spreader" is the coronation of the total nons(ci)ense in the belief system of #CoronasWitnesses.
Asymptomatic transmission 0.7%; 95% CI 0%-4.9% - could well be 0%!https://t.co/VeZTzxXfvT
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
8/8
— Dr. Thomas Binder, MD (@Thomas_Binder) March 24, 2020
By the way, who the f*** created this obviously (almost) worldwide definition of #CoronaDeath?
This is not only medical malpractice, this is utterly insane!https://t.co/FFsTx4L2mw







