Categories Health





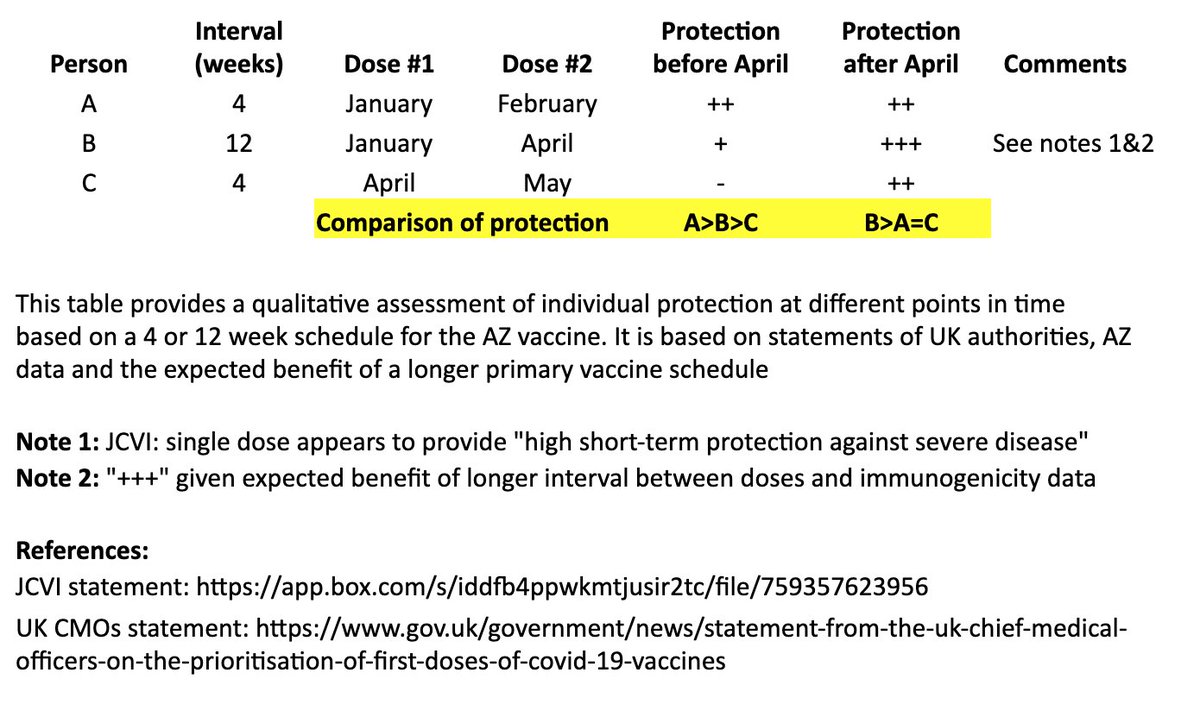
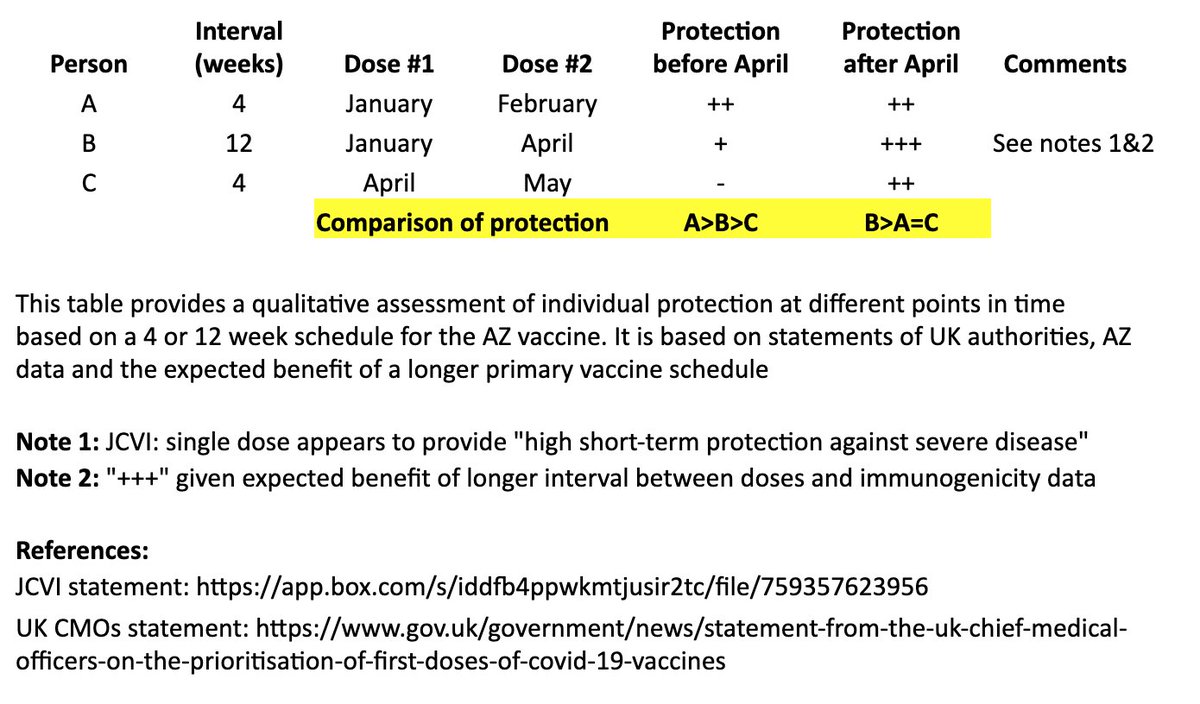
I created a simple table to illustrate the individual impact of the "flexible second dose timing" now recommended in the UK.
Coincidentally, @bob_wachter & @ashishkjha just tackled the US policy question in this important piece. 1/
https://t.co/n5bHkdIo0c
In @washingtonpost, @ashishkjha & I argue for the 2nd-shot-deferred strategy, partly by invoking the Mike Tyson principle. https://t.co/ZxrgVj3TJe We both came to this view because of the slow rollout & the new variant. But it's a tough call and reasonable people will disagree.
— Bob Wachter (@Bob_Wachter) January 3, 2021
I based this on recent statements from the UK chief medical officers, JCVI, and what we know from prior vaccine development. 2/
JCVI: https://t.co/6FQ25d6MFE
UK Chief Medical Officer (CMO) statement: https://t.co/RTpAIqgE1i
CMO letter to the profession:
This table and thread focuses on the AZ vaccine, where more data on a delayed second dose is available than with the Pfizer vaccine. It is not intended to address questions about single-dose regimens or mix & match approaches. 3/
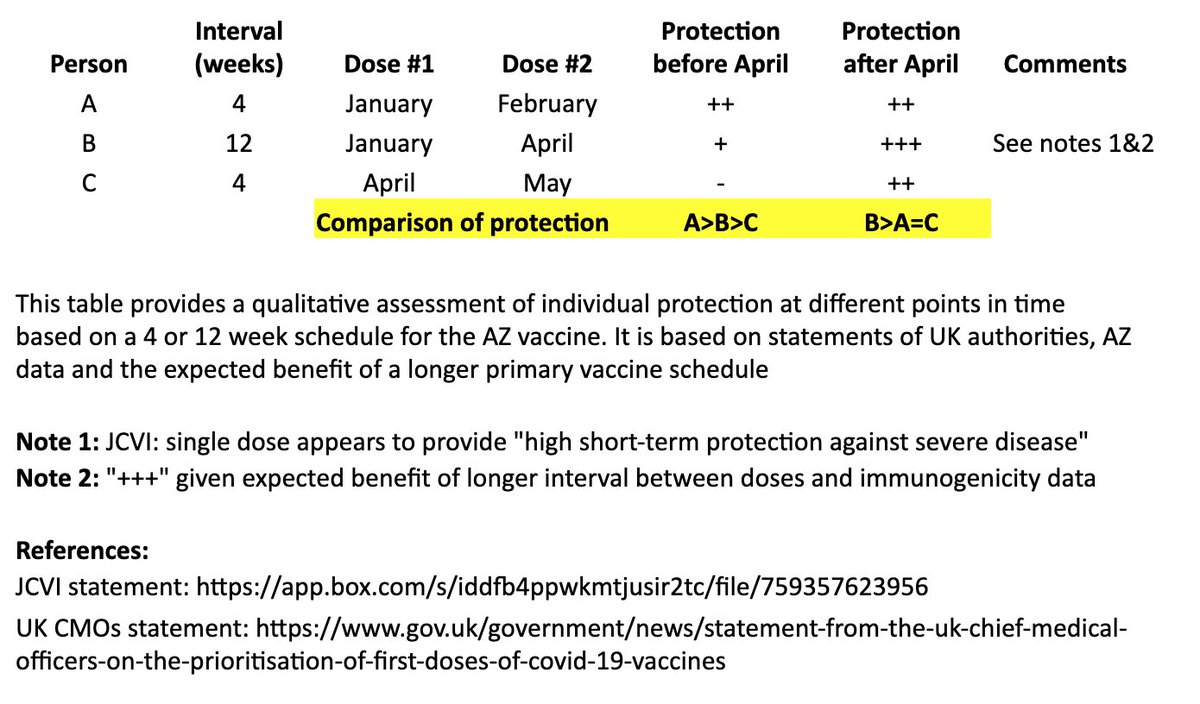
In the table, persons “A” and “B” both receive their first dose in January. “A” receives their second dose in February (4 weeks later), and “B” receives their second dose in April (12 weeks later). “C” receives their first dose in April and second dose in May (4 weeks later). 4/
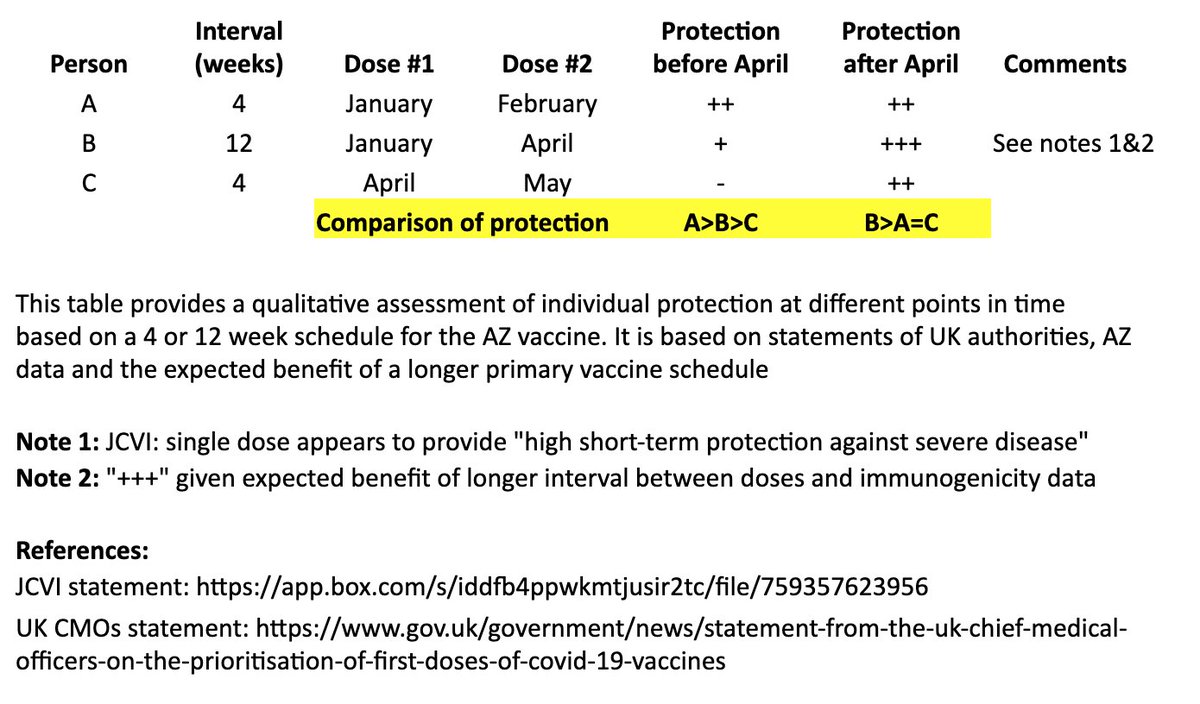
I made a qualitative comparison the potential efficacy during the two months between “A” and “B’s” second dose, as well as the potential longer-term efficacy after “B” receives their second dose. 5/












https://t.co/8amD9PQhfO
So overwhelmed. Filmed in A Cardiff Hospital (disclaimer. Not by me!) . Notice the empty beds also. \U0001f92c\U0001f92c pic.twitter.com/dZcE9cMERy
— Tracy make the world great \U0001f4ab (@TracyICQ) December 30, 2020
https://t.co/pmCsSJ6a1p
Romford Hospital - my man on the ground was there for over an hour. pic.twitter.com/jk0BxtLF5o
— Ministry Of Dissent, #EndTheLockdown #KBF (@MinistryDissent) December 30, 2020
https://t.co/KRPpFVCSgz
Don\u2019t know who this is or when it was filmed, but it raises questions #NightingaleHospitals pic.twitter.com/eyuIZuJGDz
— R Bemath (@RBemath) December 29, 2020
https://t.co/9iyvqPyo9O
Worth noting on hospital occupancy. I\u2019m hearing anecdotal evidence of same from whistleblowers in hospitals including in London. https://t.co/fahC18EbEw
— Richard Tice (@TiceRichard) December 29, 2020


What about medical culture and who is not policed on professionalism that allowed him to get so far?
Has a single physician caused more damage to the public health than British gastroenterologist Andrew Wakefield? https://t.co/W3k21Ais6F
— Harry Thomas (@DrHarryThomas) June 10, 2020
When I look at Wakefield, I see the same kind of lack of ethics evident in #Medbikini study
but Wakefield was far further down the spectrum
because he was doing invasive GI procedures on children for his study, funded by a lawyer
First: consent matters
Informed consent matters
What incentives exist in healthcare & academia that shaped his mindset & behaviors?
What was Wakefield rewarded for throughout his career?
Where did he NOT get questioned?
Look as this patent he had filed to compete vs MMR
Gibberish
+
His 🤑incentive
https://t.co/NRqXvBCGvB
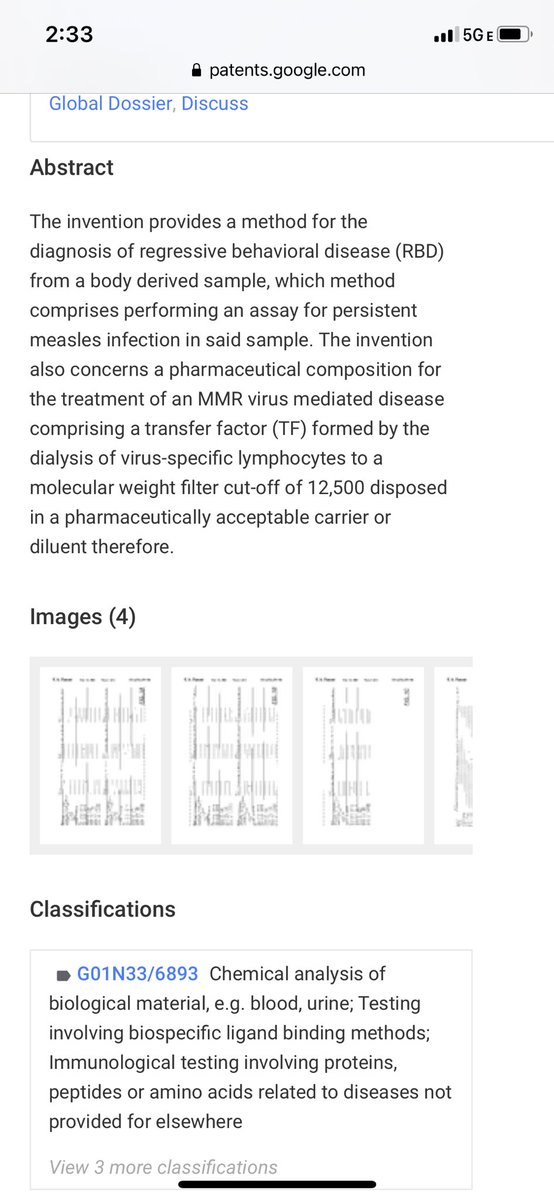
Please note in his patent application Wakefield used those 12 samples that he cited in his @TheLancet study. He was not the only author. There were reviewers. There were editors. He was not alone in a cave. He was bullying his staff too
This was NOT “one man”
And lots of silence
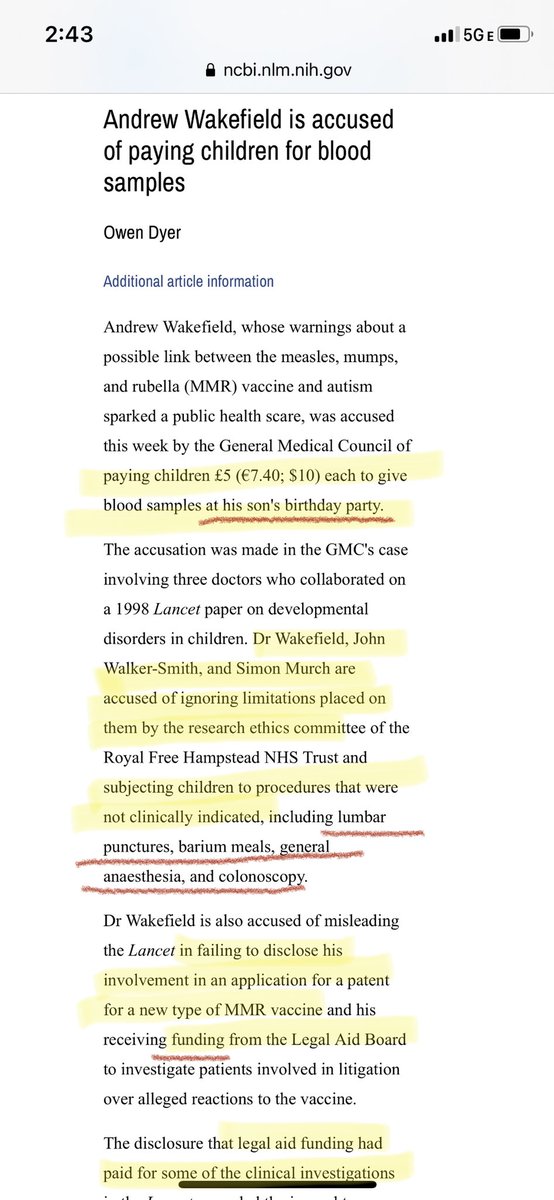
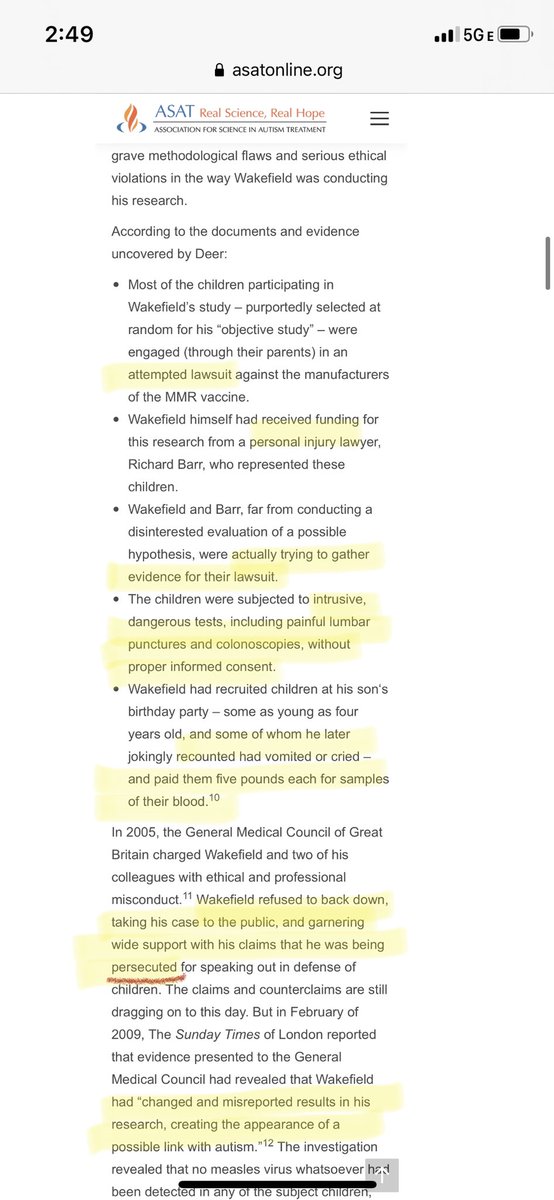
“Joking” about kids crying & vomiting? Sounds like a massive jerk.
Erased/changed data
I have a hard time believing no one found him problematic before
Were people afraid to report?
When held accountable, he catastrophized, claiming he was being “persecuted”
Sound familiar?









It's interesting that even a condition as common as #Migraine is still not well understood.
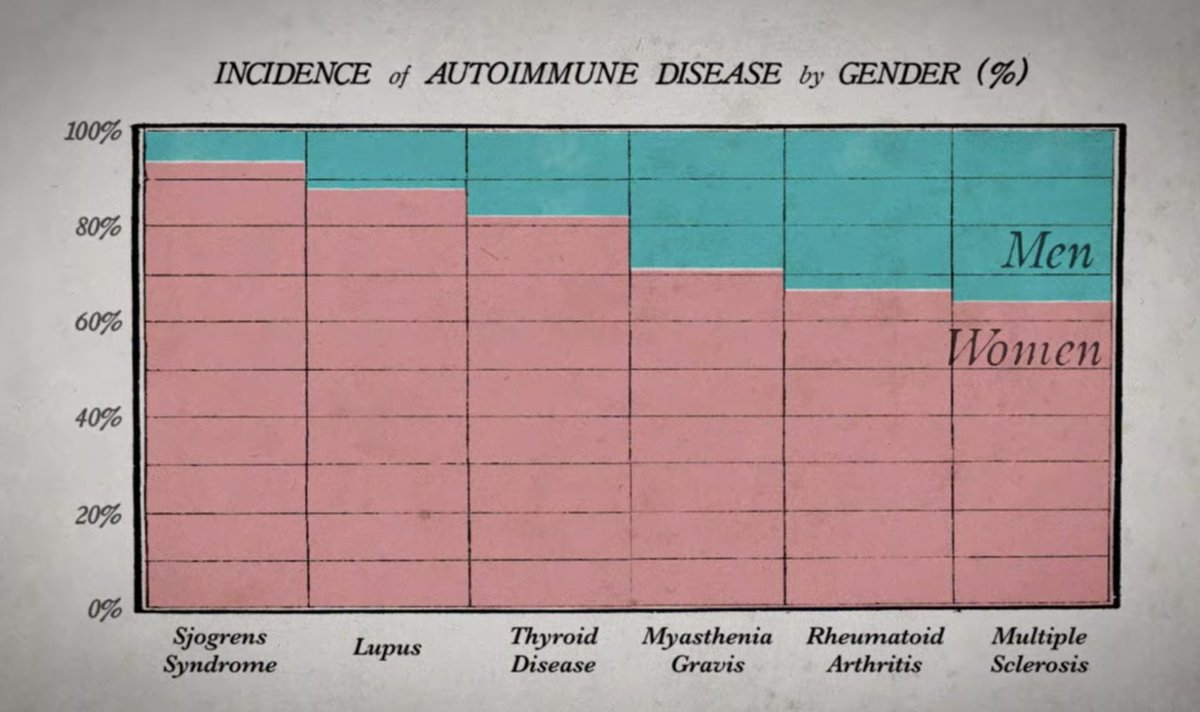
Significant overlap with many other conditions mostly impacting women that are also "not well understood" is present.
https://t.co/EhrnxfItsm https://t.co/R7QUKrZvhR
2/ As a women’s health clinician & #COVID researcher I know ME/CFS, #LongCOVID & most autoimmune diseases disproportionately impact women after puberty. Female preponderance has likely contributed to the historical neglect of funding & subsequent lack of interest in studying them
3/ Paradoxically, the ongoing dismissal of many of women’s symptoms and abuse by the medical system is a direct result of our lack of understanding & ongoing LACK of funding.
cc: @jenbrea @ahandvanish @AthenaAkrami @Dr2NisreenAlwan
If you work on #longCOVID and say \u201cI\u2019m not an #MECFS expert, I don\u2019t know anything about it, it\u2019s not my job to know about ME or \u2019fatigue\u2019\u201d then you really, REALLY need to learn about ME. This is what MANY infections can do, not just SARS2. pic.twitter.com/zke0MqwrEd
— Jennifer Brea\U0001f992 (@jenbrea) January 14, 2021
4/ This pattern of ignorance/lack of understanding and dismissal, further perpetuates the trauma women suffering from chronic illness must endure. @ahandvanish @AthenaAkrami @jenbrea @RanaAwdish @VirusesImmunity @angie_rasmussen
Example stats ME/CFS:
In ME/CFS is about 80/20 female/male. Before puberty, gender ratio is 50/50. Many anecdotal reports of trans people who take hormones: F to M improve, M to F experience worsening symptoms. Female preponderance is found in both sporadic cases and historically, in outbreaks.
— Jennifer Brea\U0001f992 (@jenbrea) January 12, 2021
5/ Or Functional Neurologic Disorder (FND) aka Conversion Disorder, Hysteria, or Psychogenic Non-Epileptic Seizures (PNES).
Majority of patients with PNES are women, outnumbering men by a ratio of 3:1. Female sex preponderance occurs after puberty & usually before the age of 55


