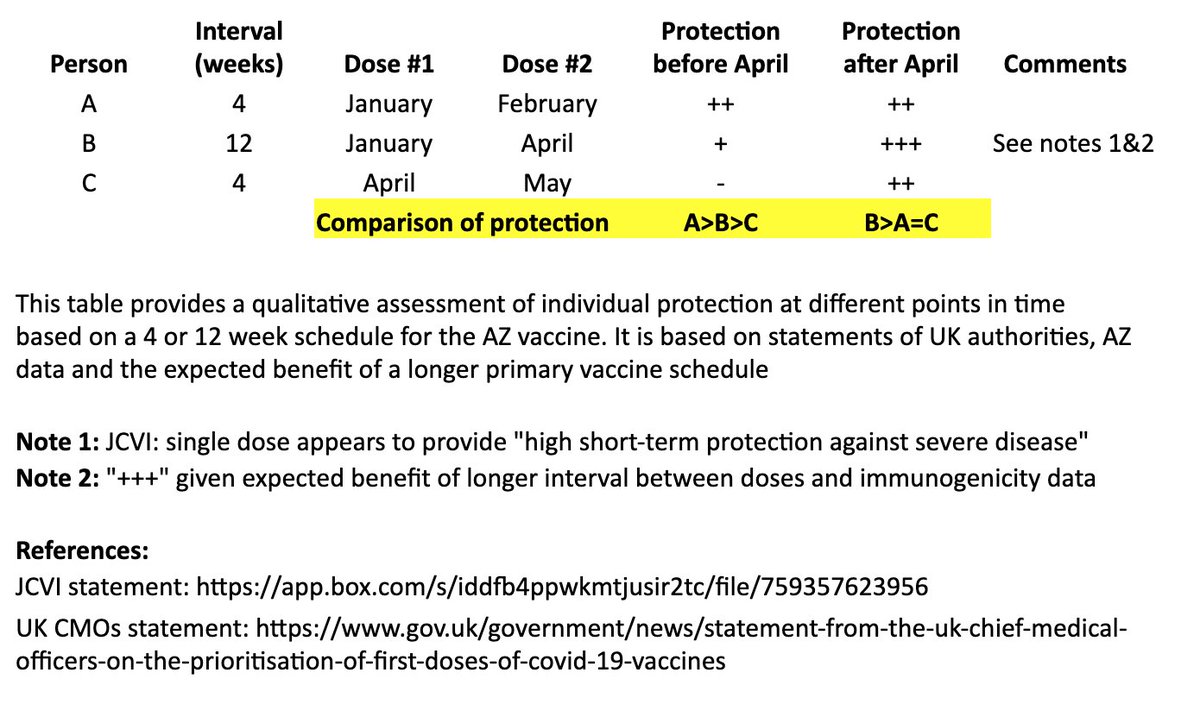
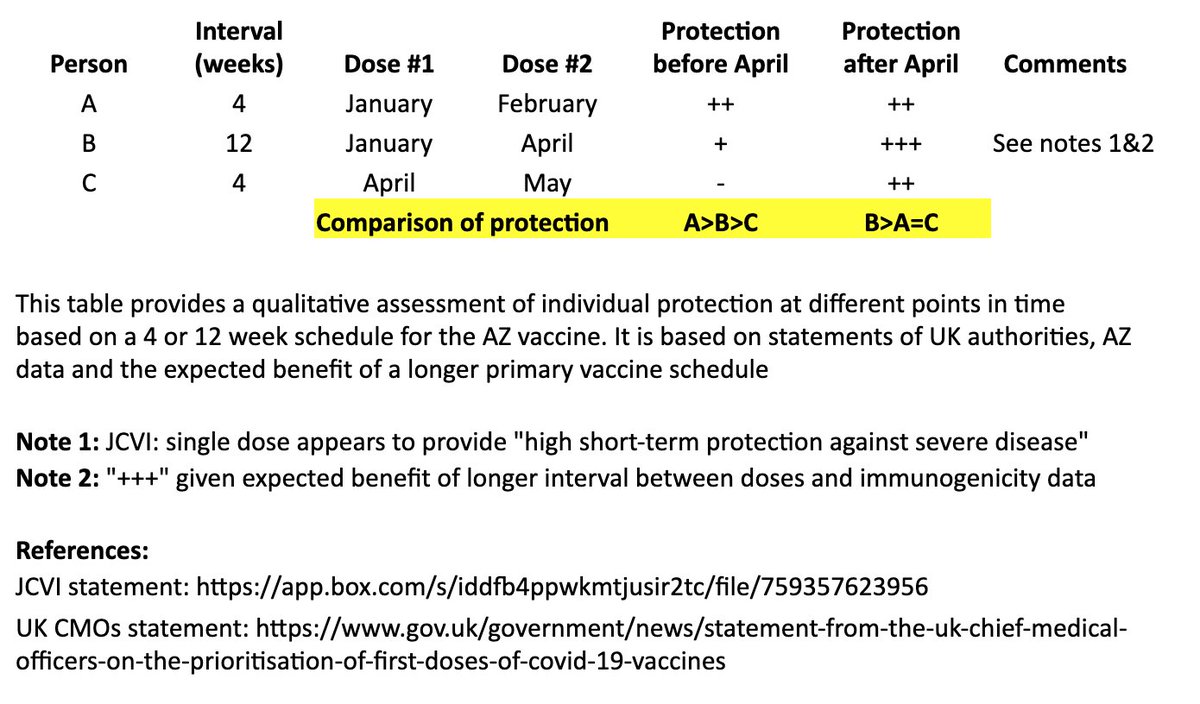
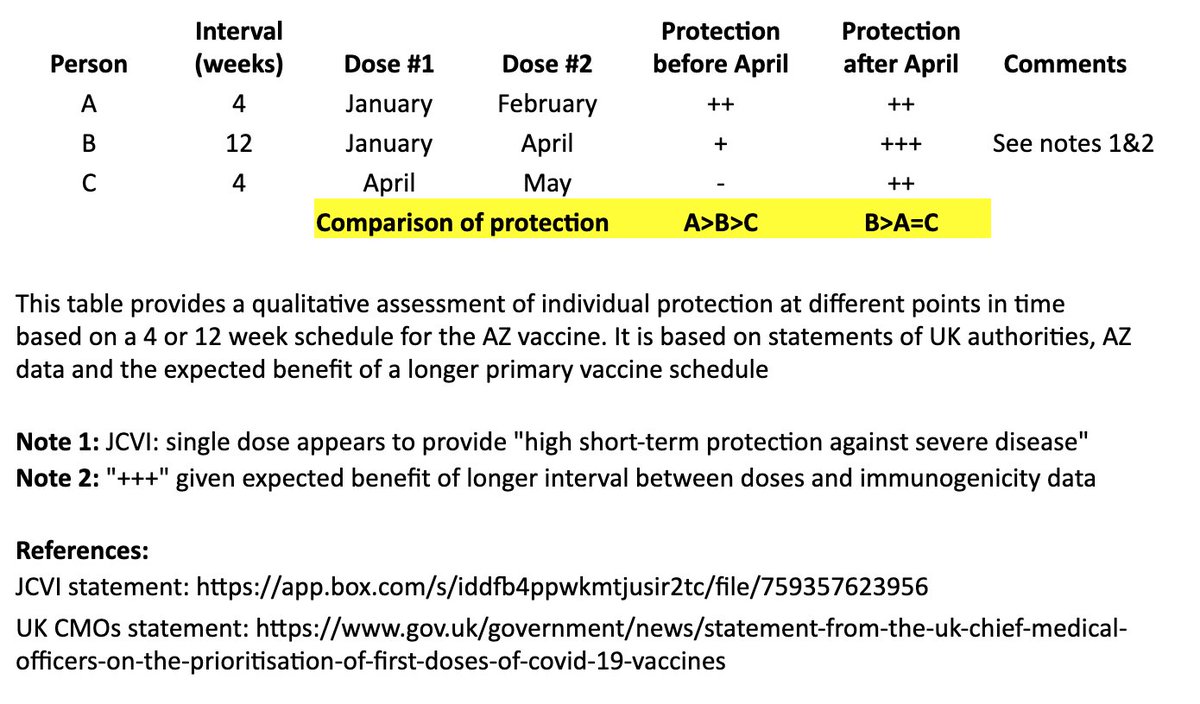
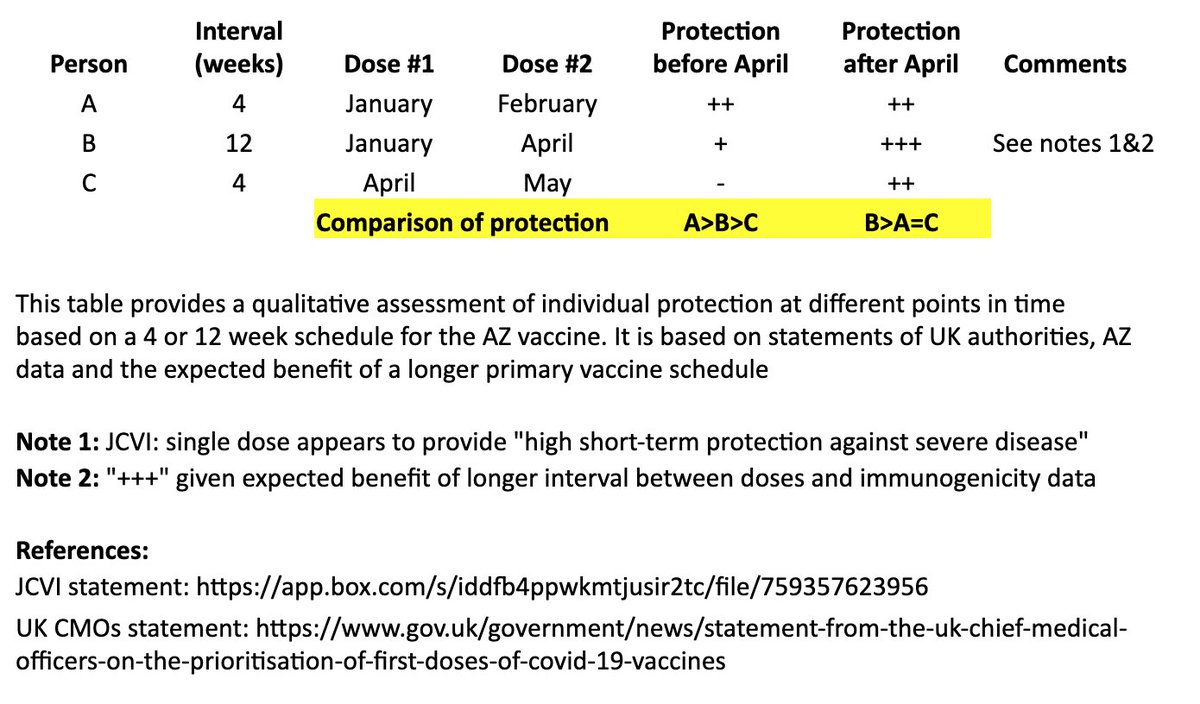
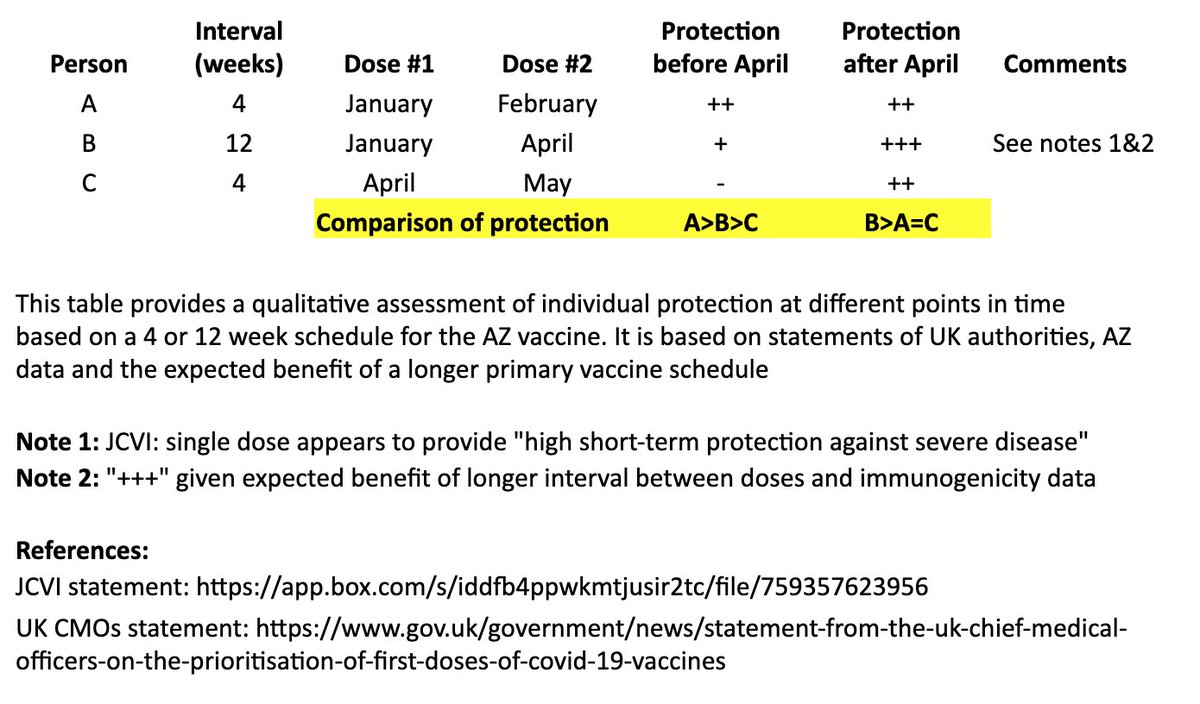
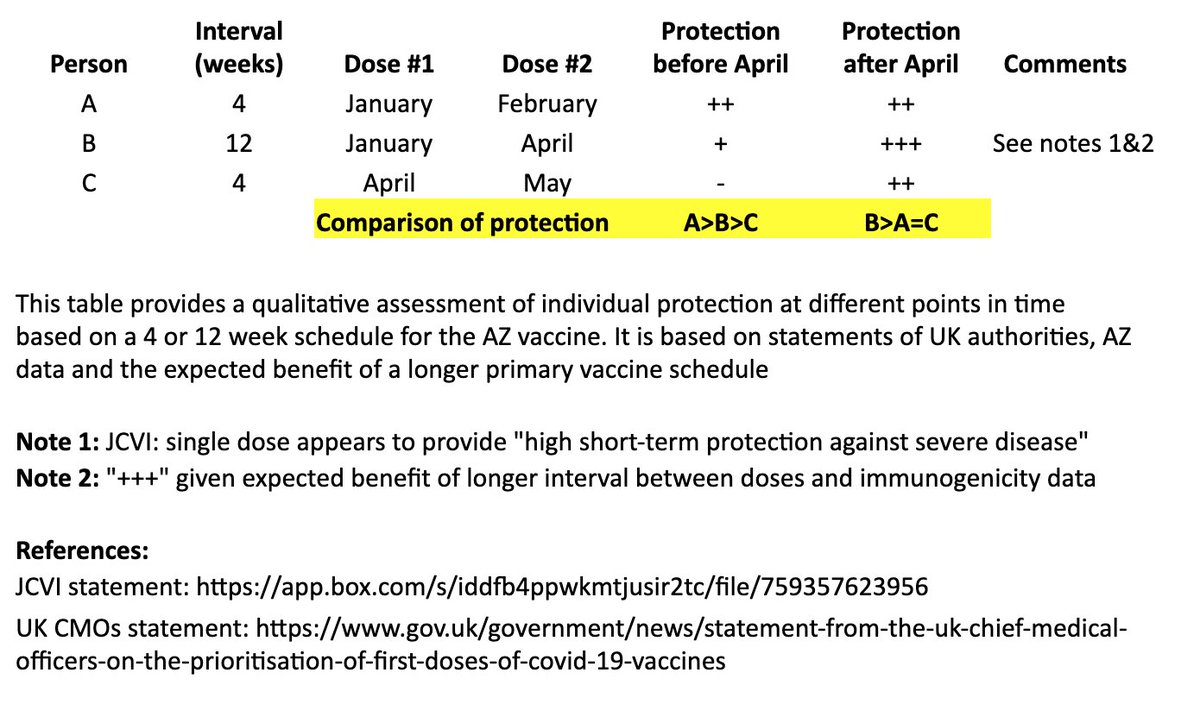
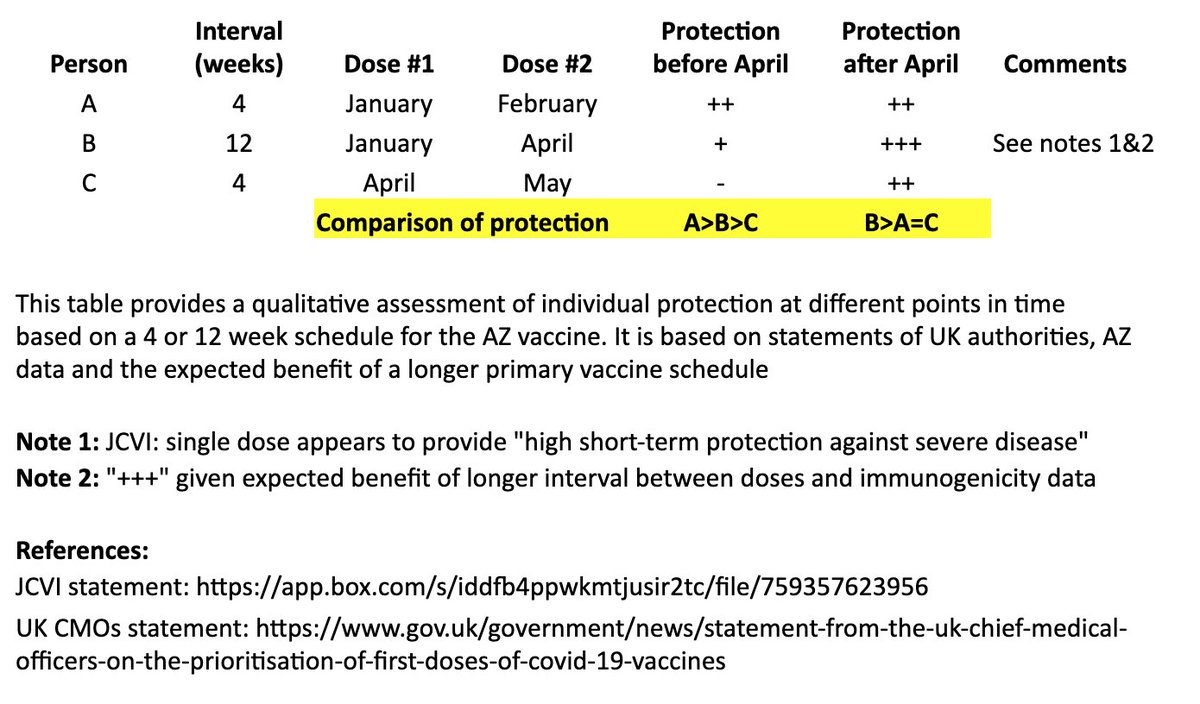
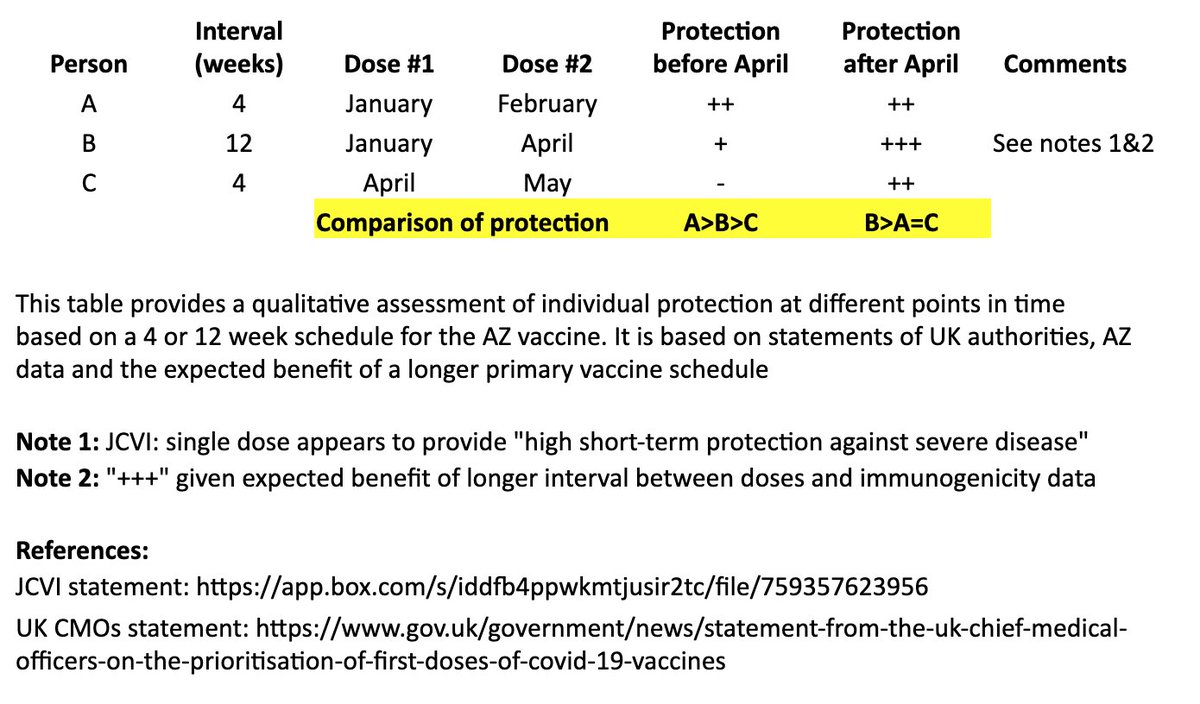
JCVI: https://t.co/6FQ25d6MFE
UK Chief Medical Officer (CMO) statement: https://t.co/RTpAIqgE1i
CMO letter to the profession: https://t.co/4WeexrVYWX
In @washingtonpost, @ashishkjha & I argue for the 2nd-shot-deferred strategy, partly by invoking the Mike Tyson principle. https://t.co/ZxrgVj3TJe We both came to this view because of the slow rollout & the new variant. But it's a tough call and reasonable people will disagree.
— Bob Wachter (@Bob_Wachter) January 3, 2021
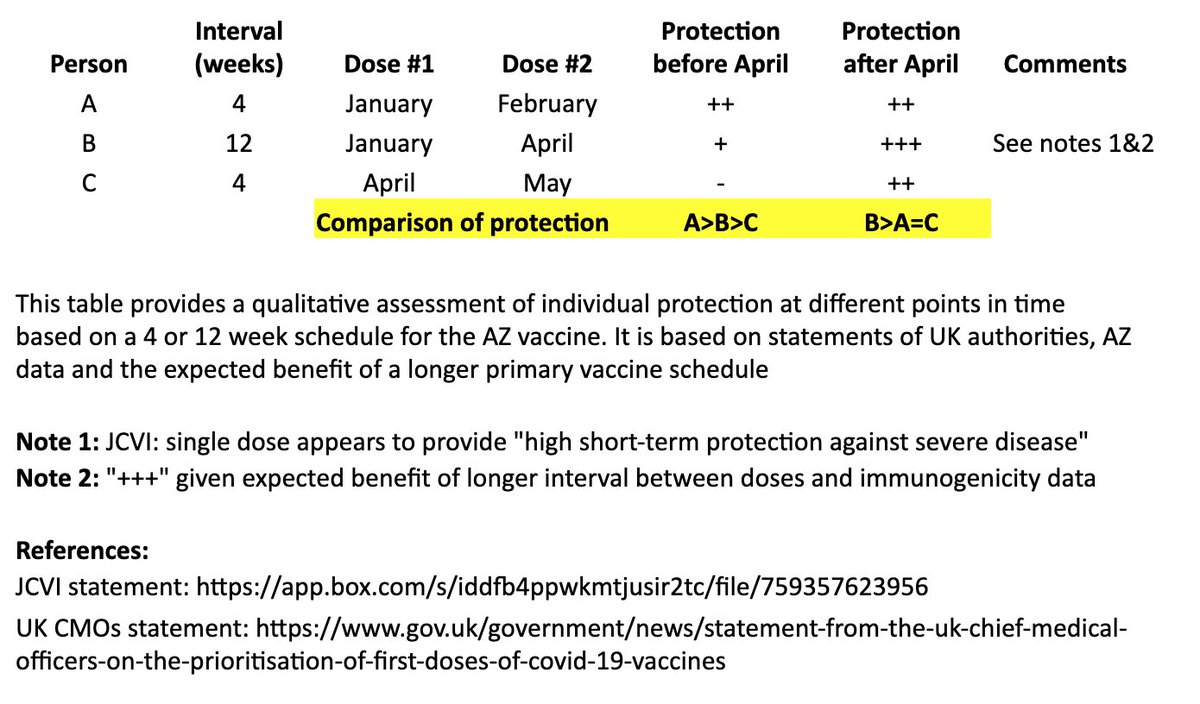
This issue is, appropriately, contentious. As a vaccinologist - & citizen & relative of people in at-risk groups - I fully support the UK decision to increase dose intervals of both our Ox/AZ product and the Pfizer product. I'd happily receive either with a >8w gap. Here's why \U0001f9f5 https://t.co/PZaxgGJUj4
— Sandy Douglas (@sandyddouglas) January 1, 2021
THREAD
— Rajeev Venkayya MD (@rvenkayya) January 1, 2021
There\u2019s much debate around the UK's recommended use of the AZ vaccine with a two-dose schedule and flexible timing of second dose. Some thoughts on the AZ recommendation (not Pfizer) based on available data with refs to some excellent threads. 1/https://t.co/IFOC9M6vkq

If the Muslim world had not existed, there literally would be no technology/achievements today.
— Starks\u262a\ufe0f\U0001f1f9\U0001f1e9 (@MegaIntelIect) January 8, 2021
Science only developed because of Islam, Europe should be grateful to Islam for civilizing their barbaric cult.
Source: The Caliph's Splendor, Pg 204-05 https://t.co/HVypO52Tpc pic.twitter.com/00jYSbaDSs



1. From Day 1, SARS-COV-2 was very well adapted to humans .....and transgenic hACE2 Mice
— Billy Bostickson \U0001f3f4\U0001f441&\U0001f441 \U0001f193 (@BillyBostickson) January 30, 2021
"we generated a mouse model expressing hACE2 by using CRISPR/Cas9 knockin technology. In comparison with wild-type C57BL/6 mice, both young & aged hACE2 mice sustained high viral loads... pic.twitter.com/j94XtSkscj
1. High Probability of serial passaging in Transgenic Mice expressing hACE2 in genesis of SARS-COV-2!
— Billy Bostickson \U0001f3f4\U0001f441&\U0001f441 \U0001f193 (@BillyBostickson) January 2, 2021
2 papers:
Human\u2013viral molecular mimicryhttps://t.co/irfH0Zgrve
Molecular Mimicryhttps://t.co/yLQoUtfS6s https://t.co/lsCv2iMEQz