⚡️Arterio-venous (AV) Access
causes significant morbidity & mortality in patients on hemodialysis
⚡️Most AV access associated complications are due to vascular stenosis👇🏽
2/
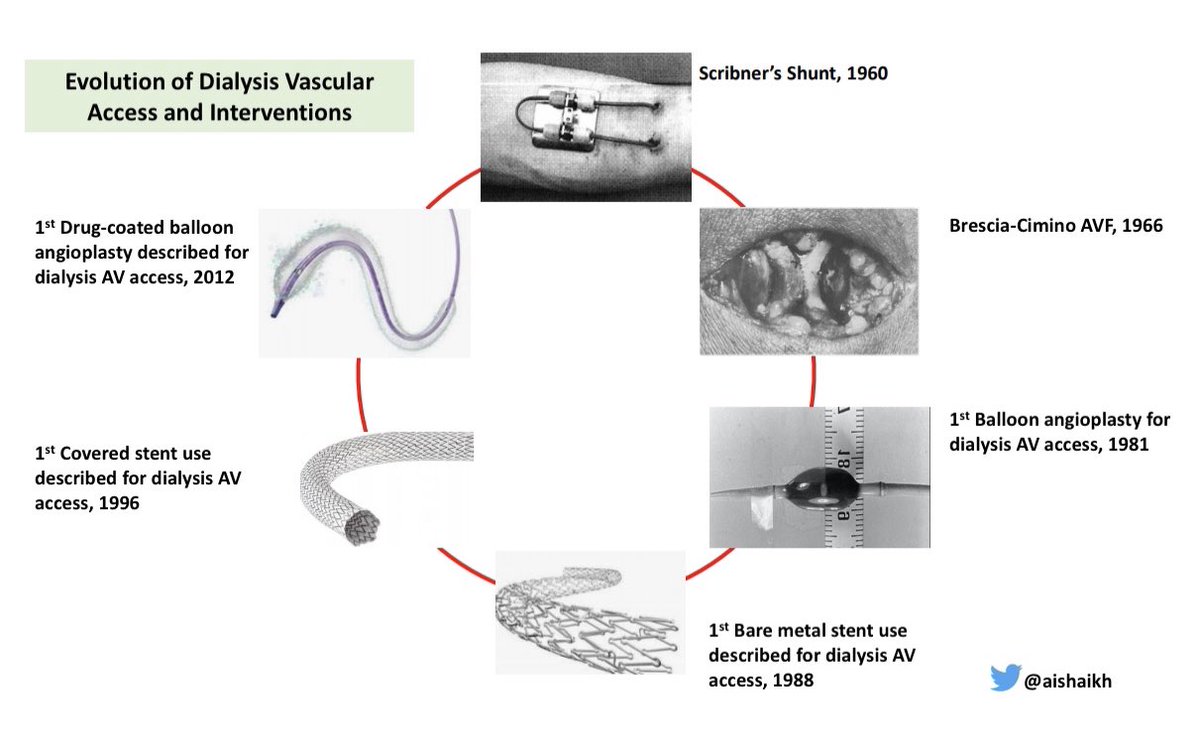
⚡️Vascular Access care has evolved over the past 60 years:
-Scribner’s Shunt in 1960 ➡️
-Brescia-Cimino AVF in 1966 ➡️
-1st Balloon Angioplasty in 1981 ➡️
-1st Bare Metal Stent in 1988 ➡️
-1st Covered Stent in 1996 ➡️
-DCB use in 2012
3/
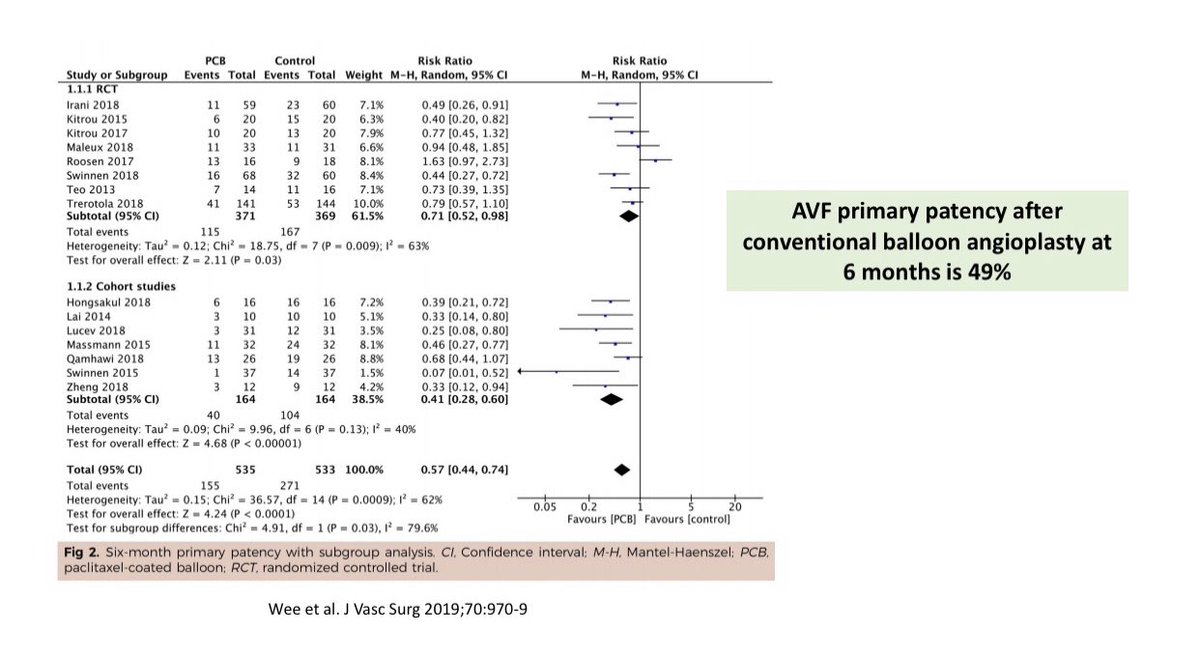
⚡️Despite these innovations, AV access stenosis remains a big problem
-Percutaneous Balloon Angioplasty (PTA) remains the 1st line therapy for stenosis but it is NOT very effective
-AVF patency after PTA is only 50% at 6-months & it is worse for AVGs👇🏽
4/
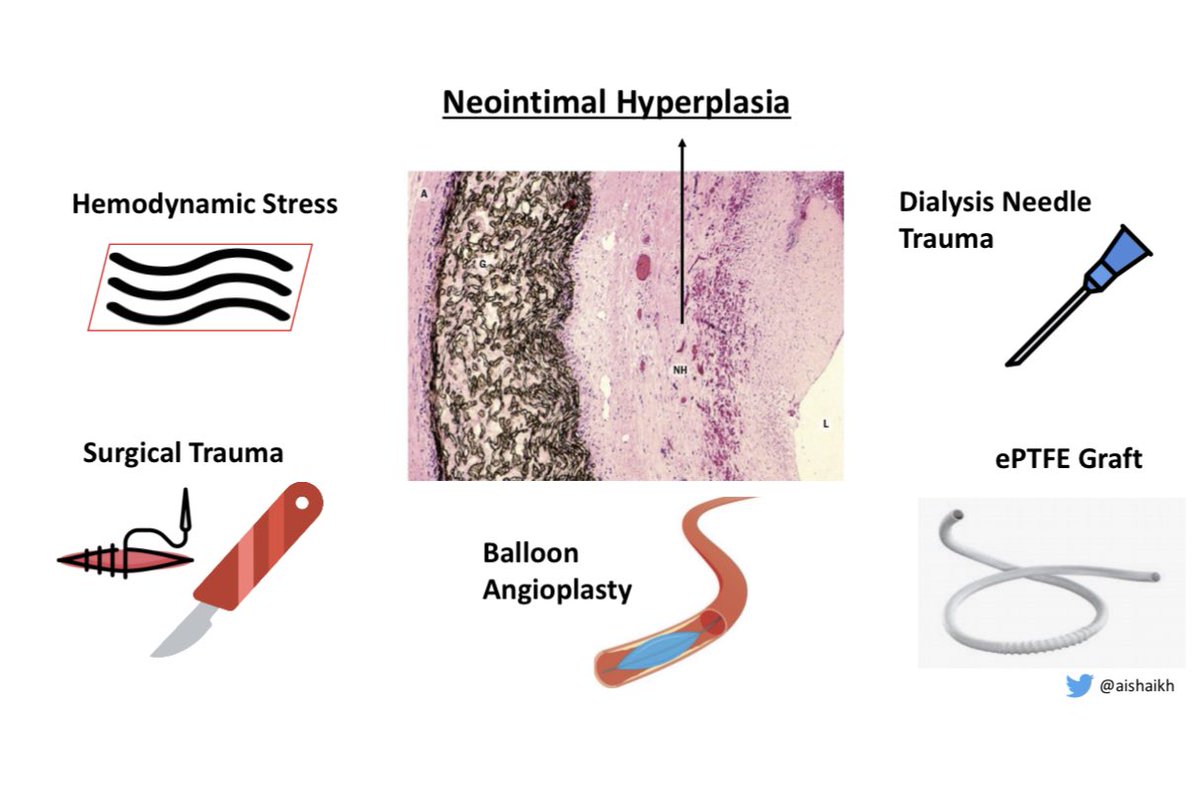
⚡️Neointimal Hyperplasia (NIH) causes vascular stenosis & it is due to:
-Hemodynamic stress
-Surgical trauma
-Cannulation needle trauma
-AVG
‼️But balloon angioplasty, the treatment for stenosis, can itself induce NIH & cause restenosis👇🏽
5/
⚡️Therefore, Endovascular Stents have been used to treat the vascular stenosis
⚡️What are Endovascular Stents?
They are scaffolds that provide mechanical endoluminal support to the vessel wall to maintain patency
6/
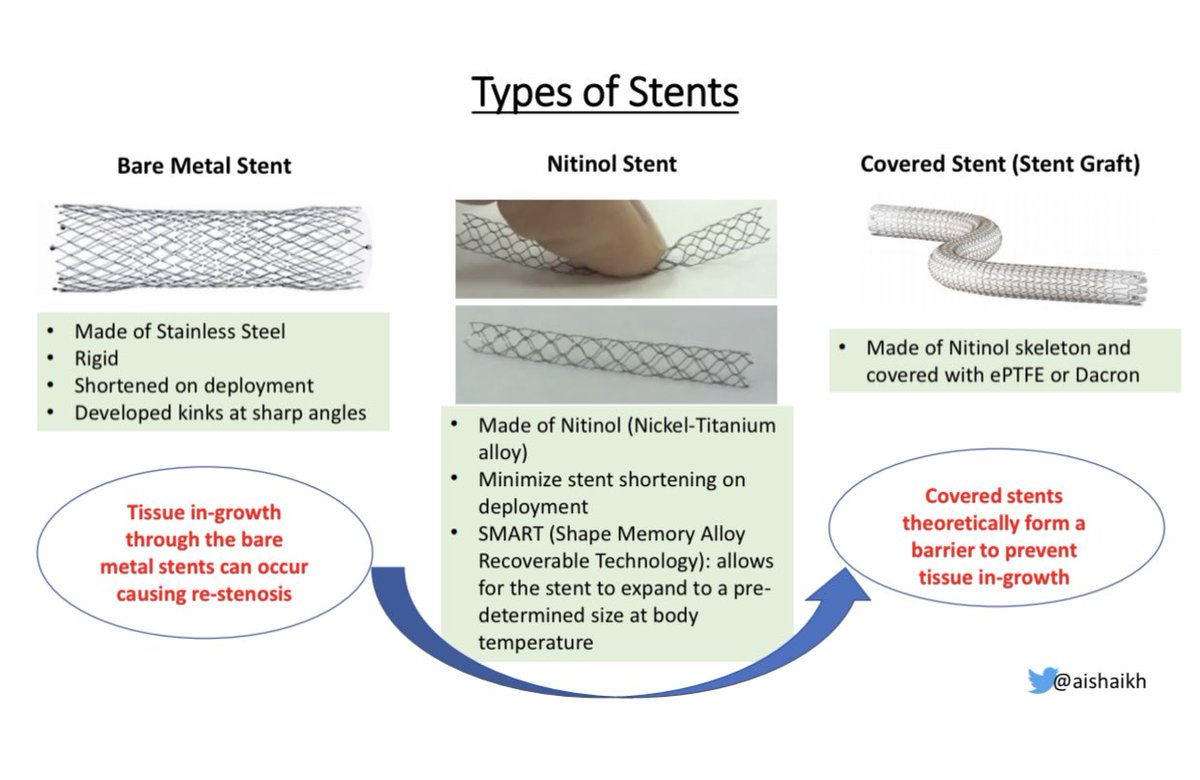
⚡️Types of Stents:
-1st generation stents were Bare-Metal Stents made of stainless steel
-Next generation of metal stents were Nitinol Stents made of nickel-titanium alloy
- Covered-Stents (Stent-Grafts) are Nitinol stents covered w/ ePTFE or Dacron
7/
⚡️Bare Metal Stents & Nitinol Stents have problems because the tissue in-growth through the bare metal causes restenosis
⚡️Covered Stents (Stent-Grafts) theoretically form a barrier, & prevent tissue in-growth through the stent & cause less restenosis👇🏽
8/
⚡️Recent clinical trials have tested the efficacy of Stent-Grafts for AV access stenosis
⚡️But before we get to the trials, let’s discuss the basic indications for Stent use:
☄️Rupture of the vessel
☄️Recoil (Residual stenosis)
☄️Restenosis
9/
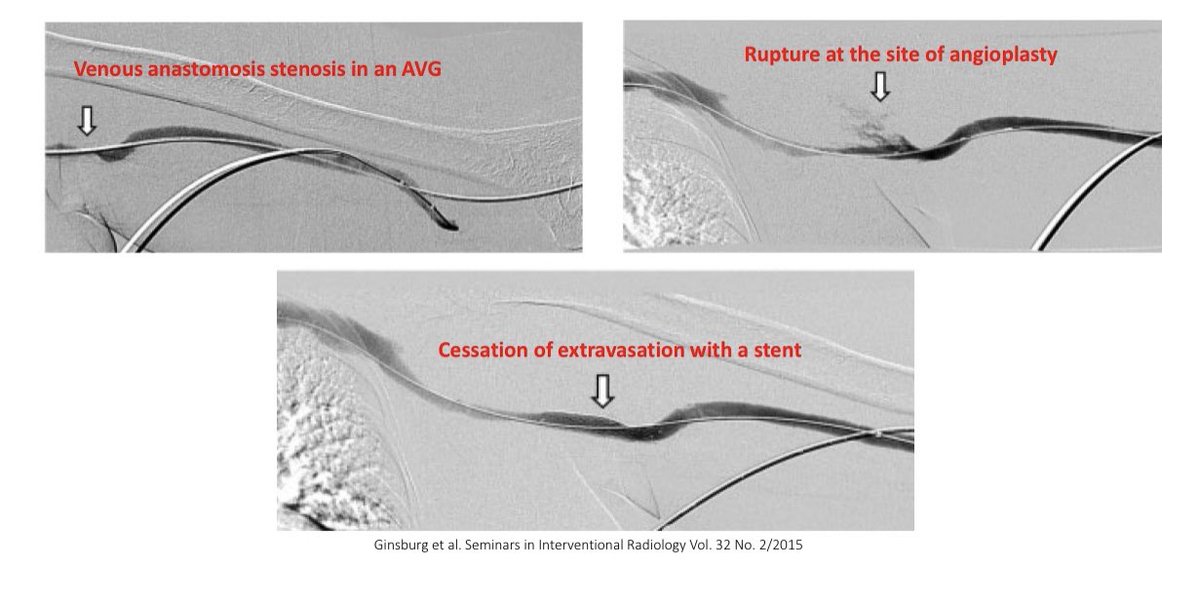
⚡️Rupture of the vessel can occur during angioplasty of a severely stenotic lesion
⚡️In most cases, extravasation can be controlled w/ manual compression or balloon tamponade but if bleeding persists then stents can be used to control the bleeding👇🏽
10/
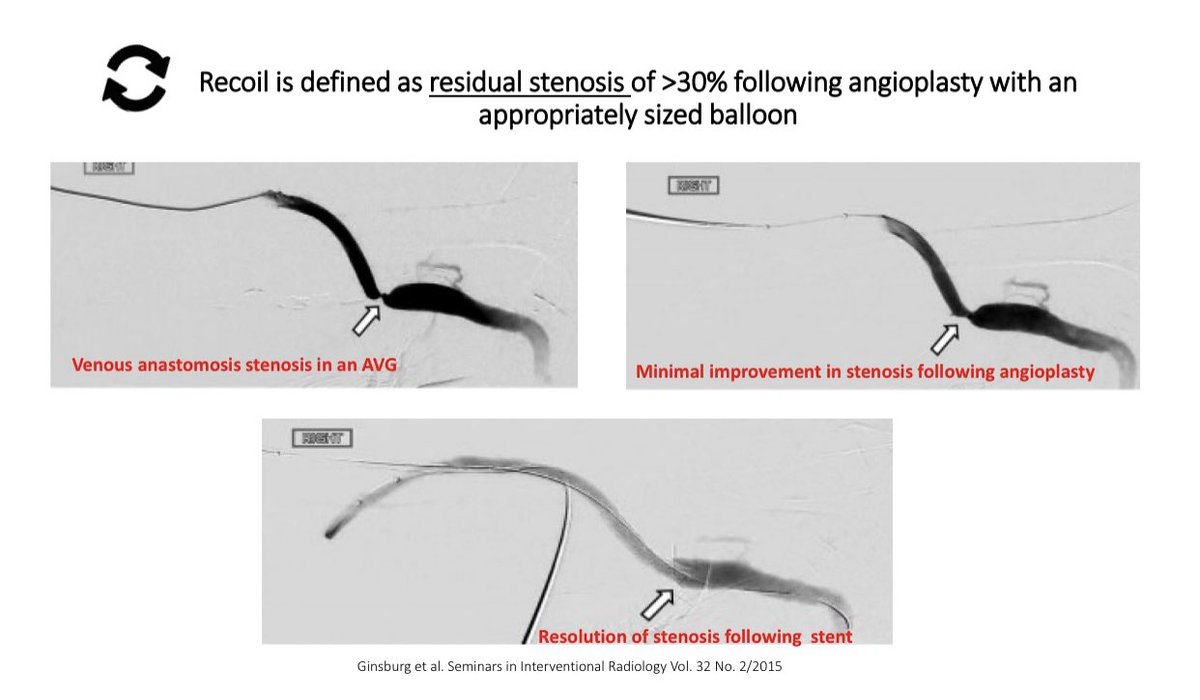
⚡️Another indication for Stent use is Recoil
⚡️Recoil is defined as residual stenosis of > 30% following angioplasty & is thought to occur due to elastic recoil of the vessel wall
⚡️Recoil is associated w/ poor AV access survival👇🏽
11/
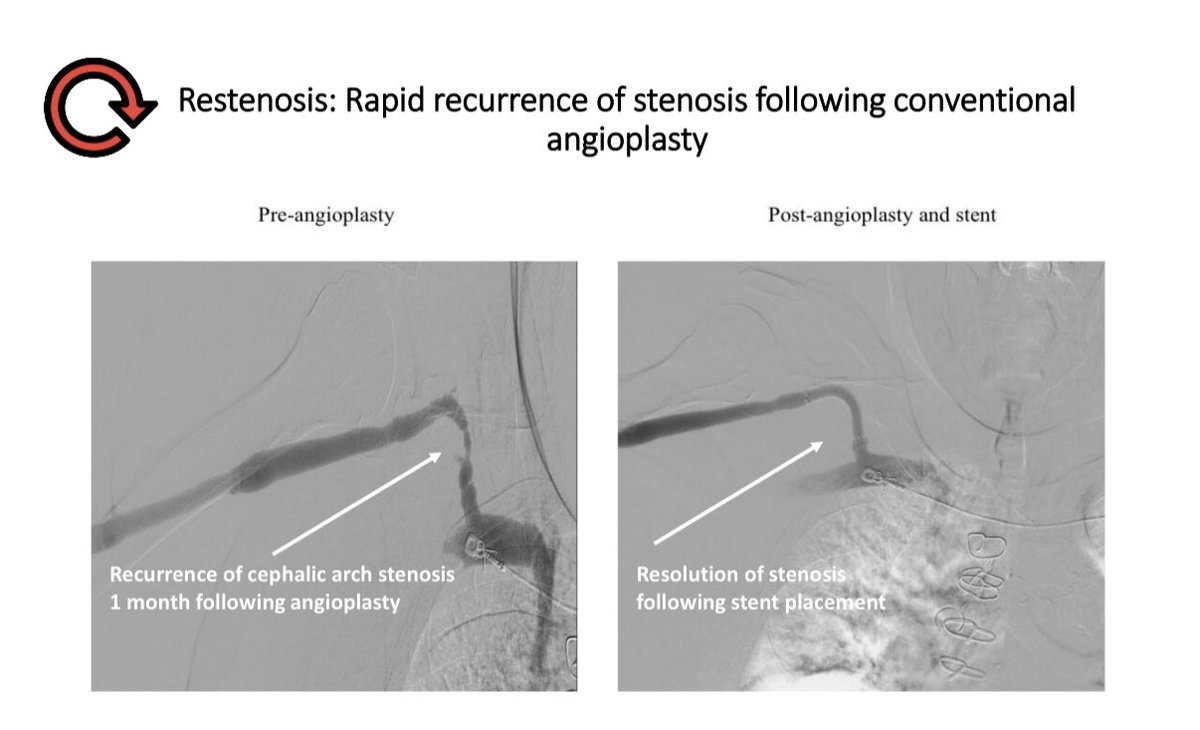
⚡️Restenosis is the most common indication for stent use👇🏽
⚡️AVG patency post-angioplasty is very poor👇🏽
⚡️Most common site for AVG stenosis is at the graft-vein anastomosis, therefore recent clinical trials have tested the Stent-grafts at this site👇🏽
12/
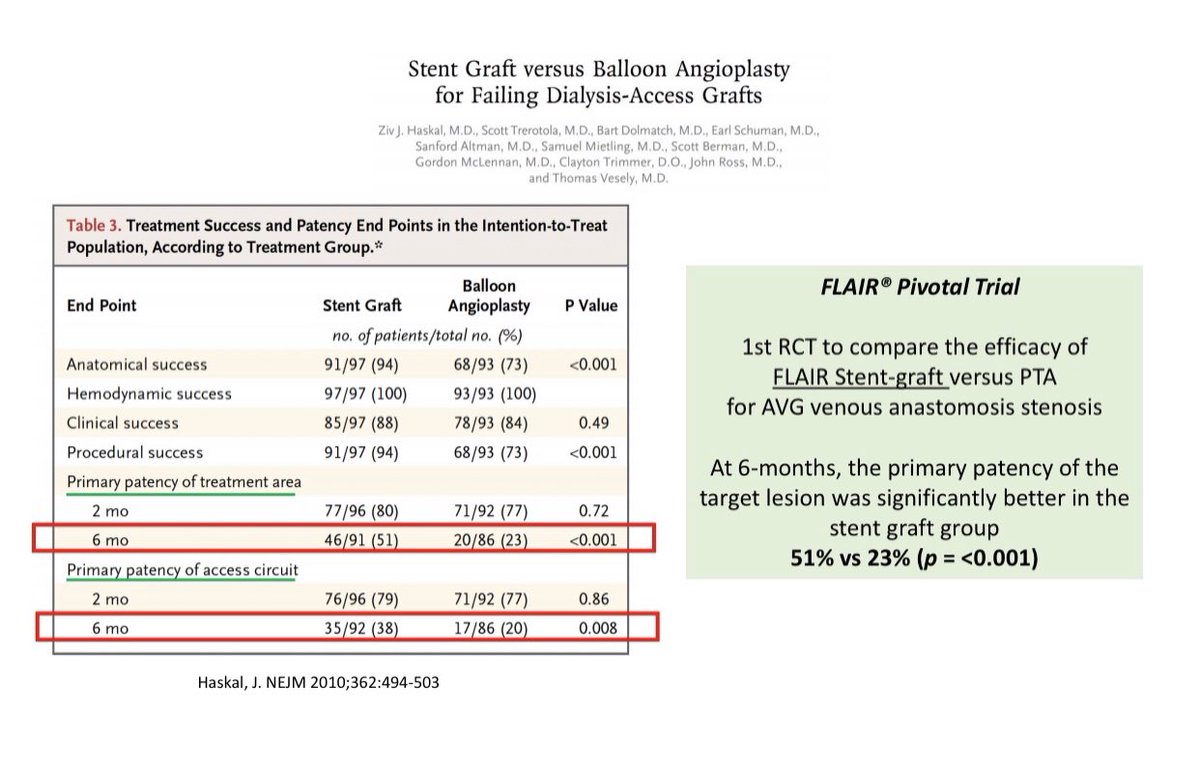
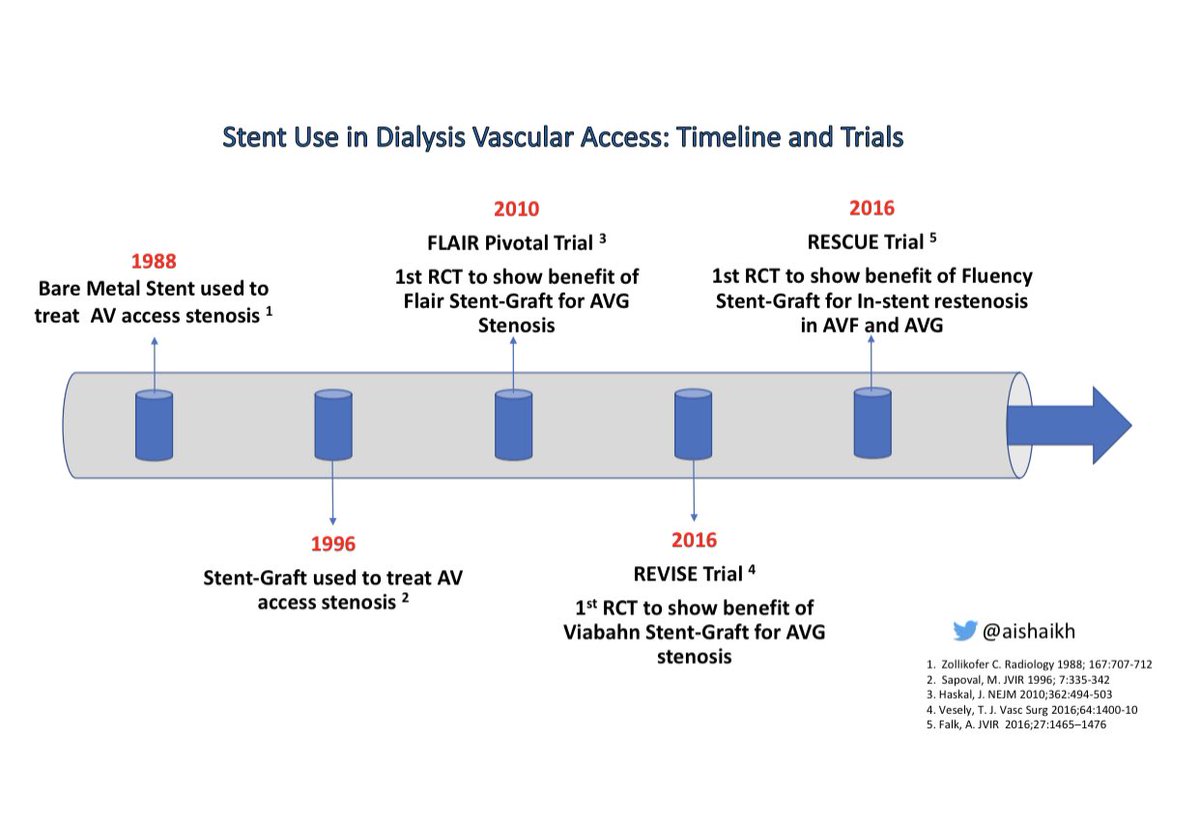
⚡️Stent-Graft (SG)Trials in Dialysis Vascular Access
☄️Flair PIVOTAL Trial: Flair SG vs. PTA for AVG
☄️REVISE Trial: Viabahn SG vs PTA for AVG
⚡️Both trials showed better 6-month patency with SG use compared to PTA for graft-vein anastomosis stenosis👇🏽
13/
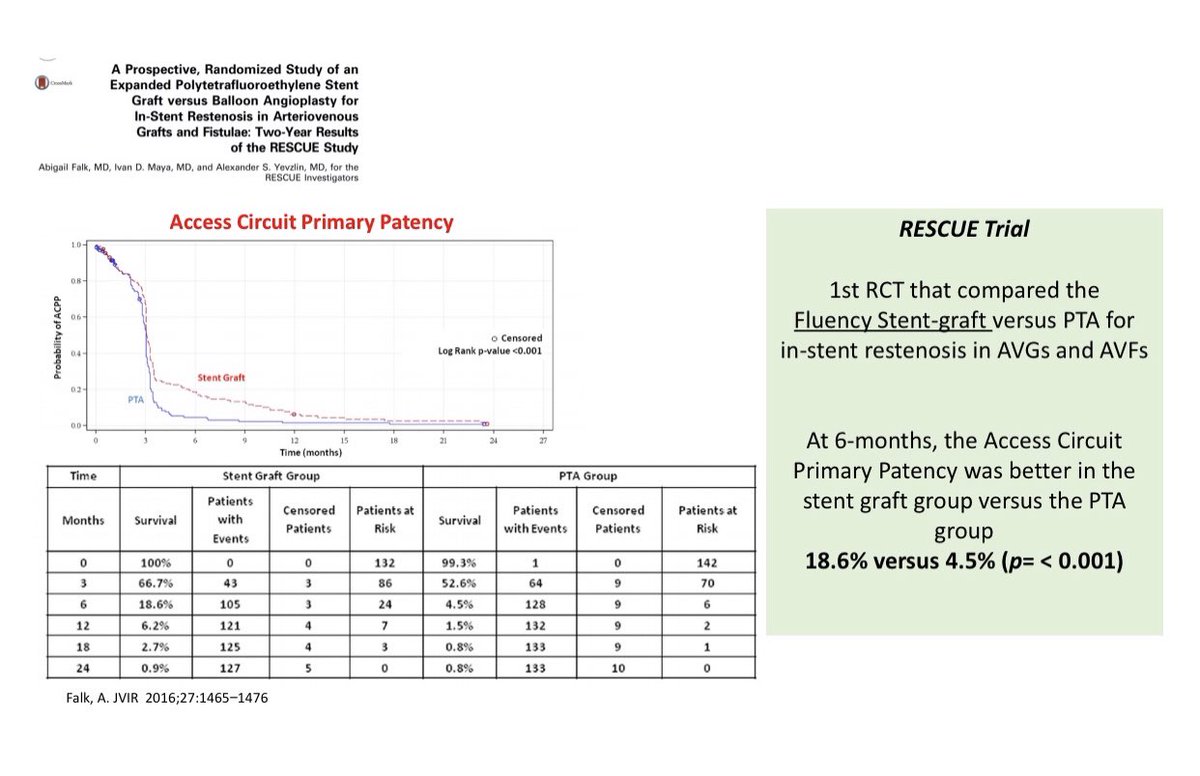
⚡️Stent-Grafts (SG) have also been tested for In-stent restenosis
☄️RESCUE Trial: Fluency SG vs PTA for In-stent restenosis in both AVF & AVG
⚡️RESCUE Trial showed better 6-month patency with SG compared to PTA👇🏽
14/
⚡️Summary of Stent Trials in Dialysis Vascular Access👇🏽
15/
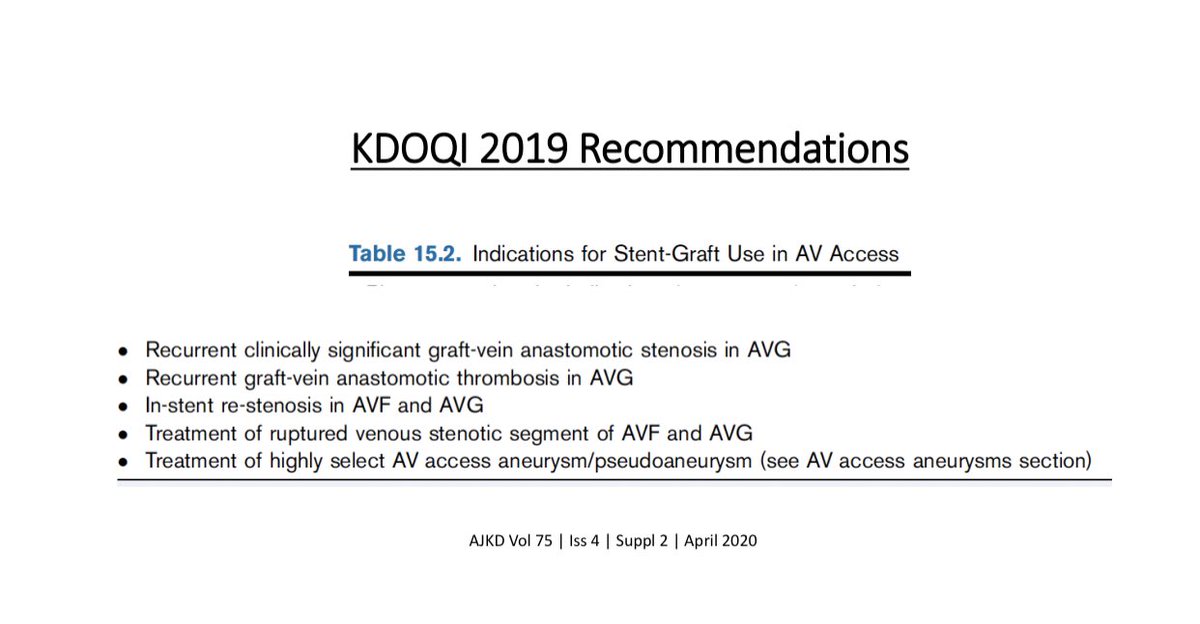
⚡️Based on this data, KDOQI 2019 guidelines recommend Stent-Graft use for:
☄️Recurrent graft-vein anastomosis stenosis in AVG
☄️In-stent restenosis in AVF & AVG👇🏽
16/
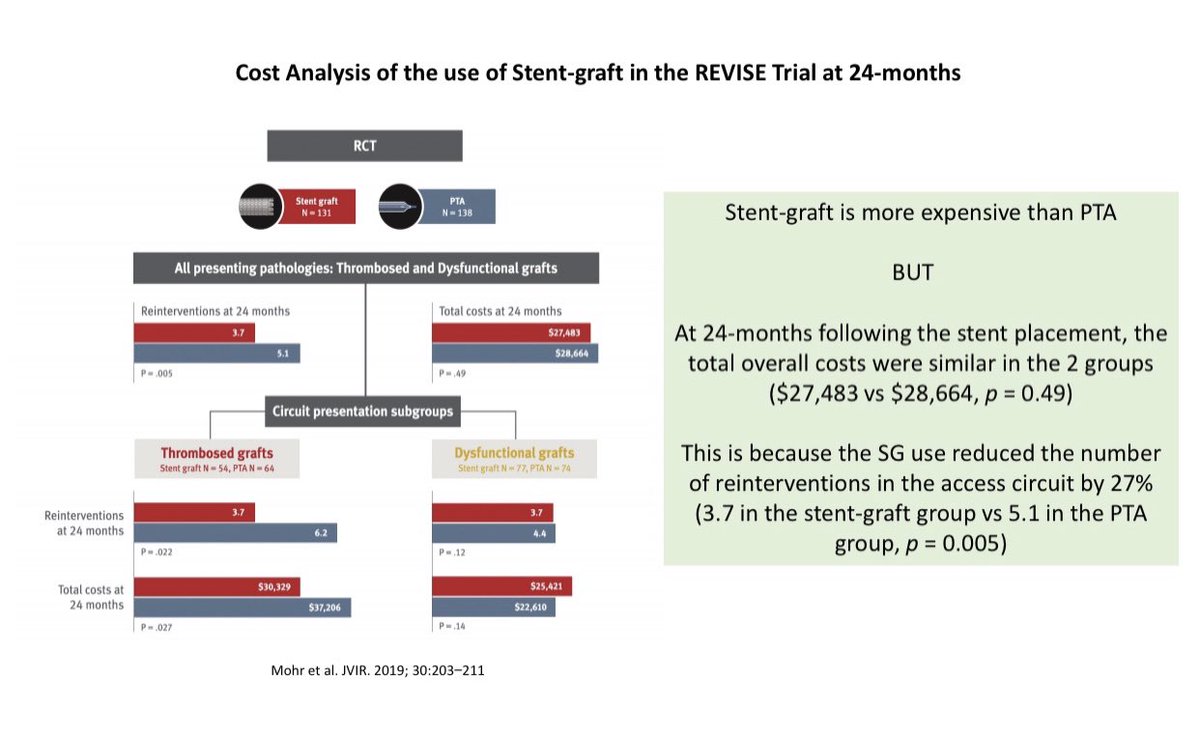
⚡️Cost analysis of Stent-Grafts (SG) show that even though the initial cost of the SG is higher than the cost of balloon angioplasty, the overall cost was similar in the 2 groups at 24-months because the re-intervention rate was lower in the SG group👇🏽
17/
⚡️Complications associated with Stent use:
☄️Stent Migration
☄️Stent Fracture
☄️Stent Strut Protrusion
☄️Jailing of the veins
☄️Infection
18/
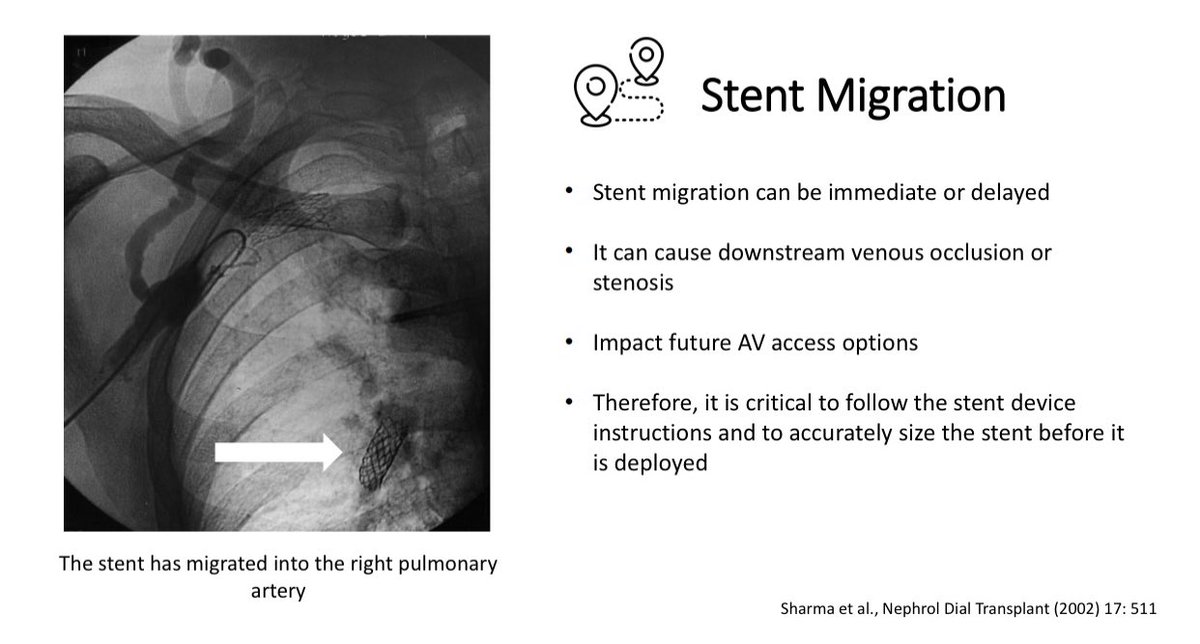
⚡️Stent Migration can cause downstream vein occlusion/stenosis & can impact future AV access options
⚡️Stent fracture & protrusion can occur due to repeated cannulation thru the stent👇🏽
⚡️Stent fracture can occur if stent is placed across a joint👇🏽
19/
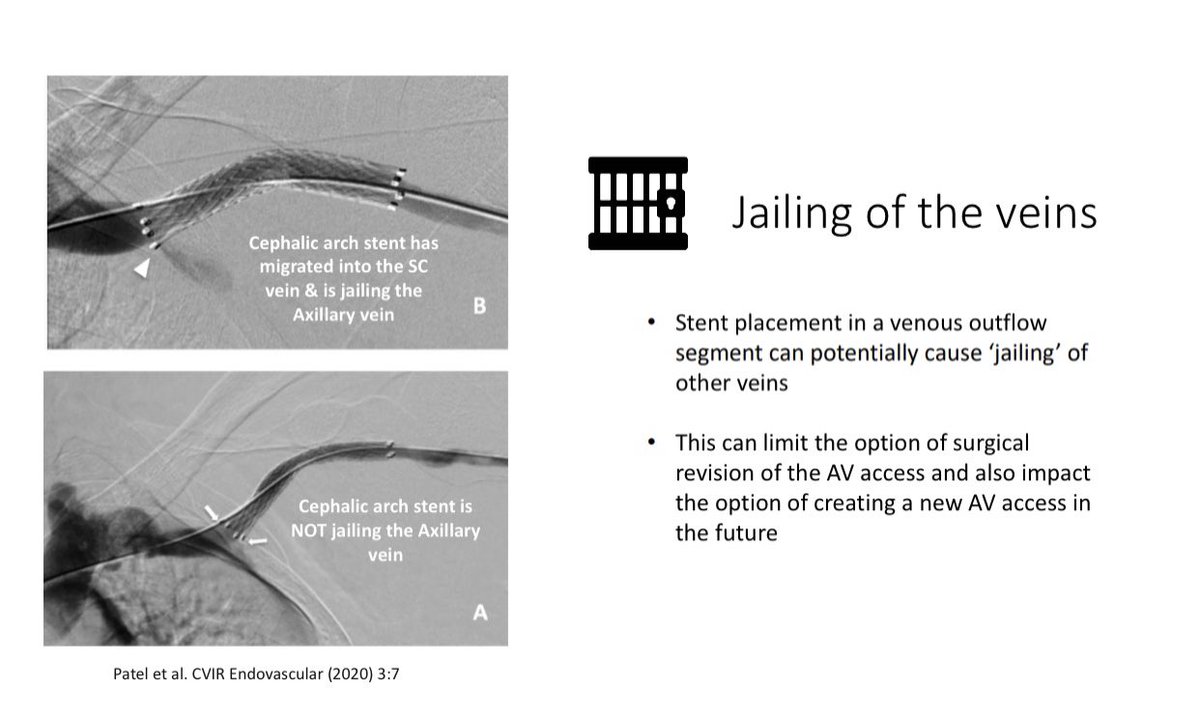
⚡️Jailing of the Veins is a complication of stent placement & this can impact future AV access options
⚡️Hence, the operator must be very careful during stent deployment in order to avoid this complication👇🏽
20/
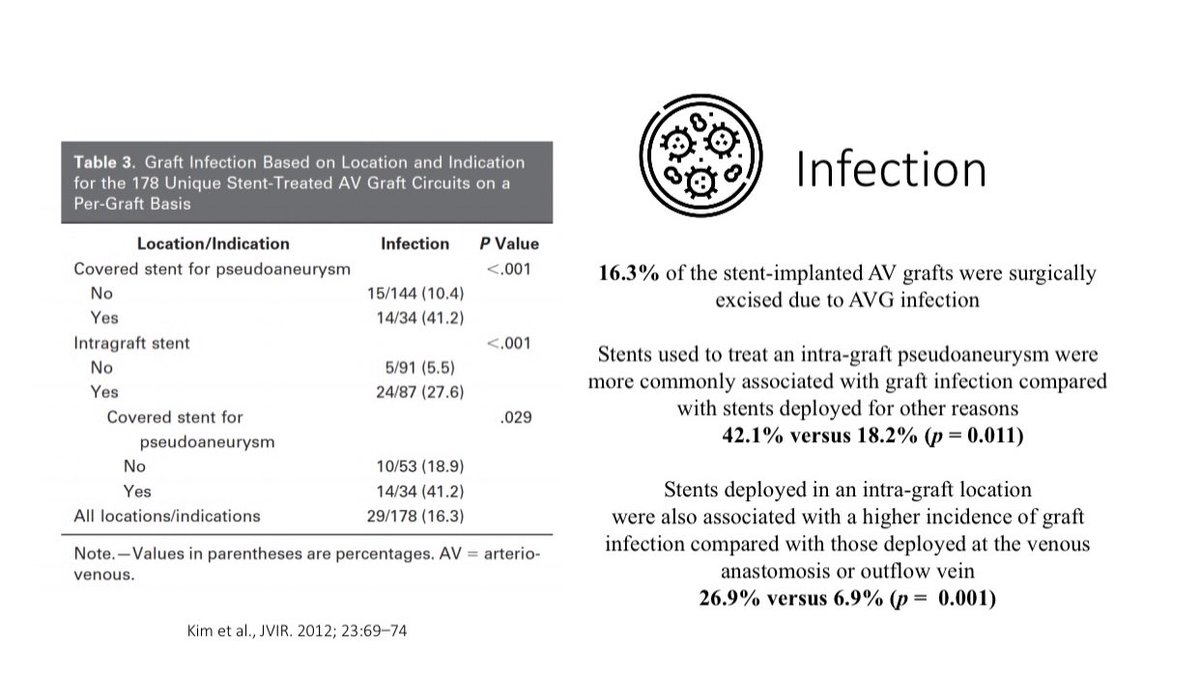
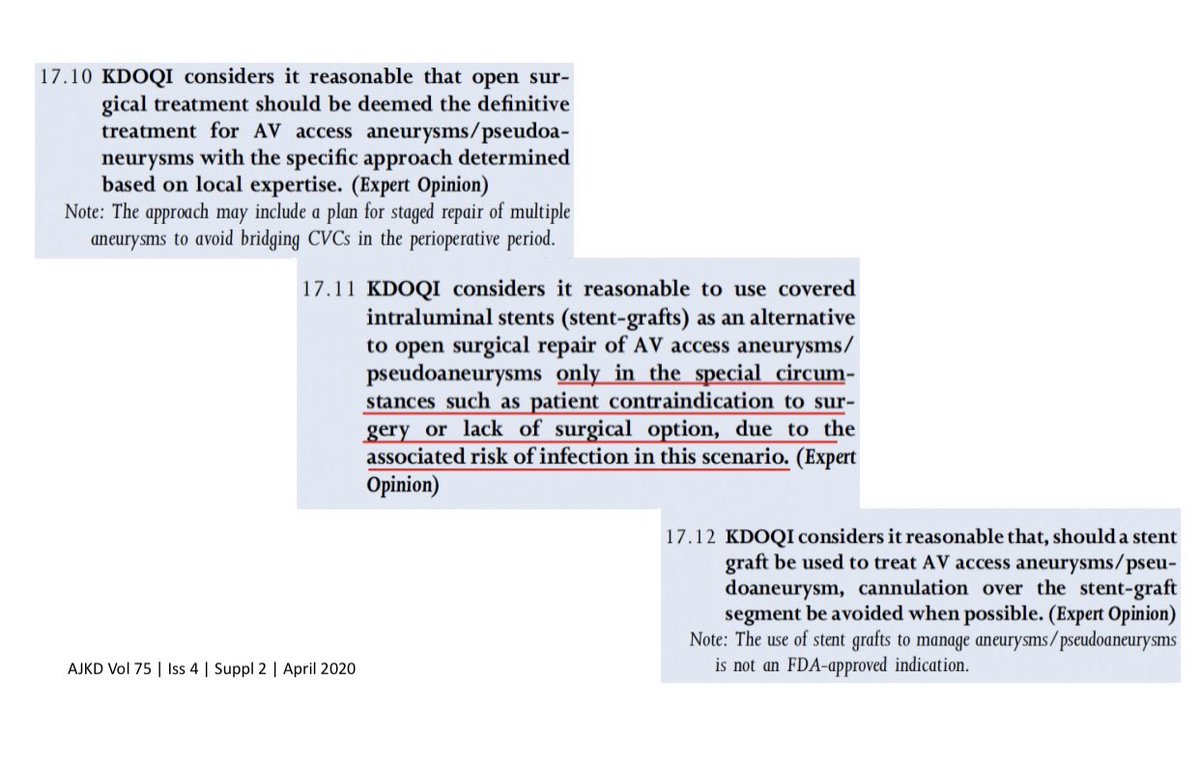
⚡️Stent associated infection is a serious complication & may require AV access excision
⚡️Stent associated AV access infections are more common when the stents are placed in the Pseudo-aneurysms 👇🏽
21/
⚡️Stent placement must be avoided in pseudo-aneurysms & in the cannulation zone due to high risk of infection & risk of stent fracture from needle trauma
⚡️KDOQI Guidelines state that stent placement for pseudo-aneurysm only be used as a ‘last resort’👇🏽
22/
💥Summary
⚡️Stent-Grafts are a viable therapeutic option for AV access stenosis but it’s use must be guided by scientific evidence
⚡️Balloon angioplasty remains the 1st line therapy for the majority of the AV access stenotic lesions
End/