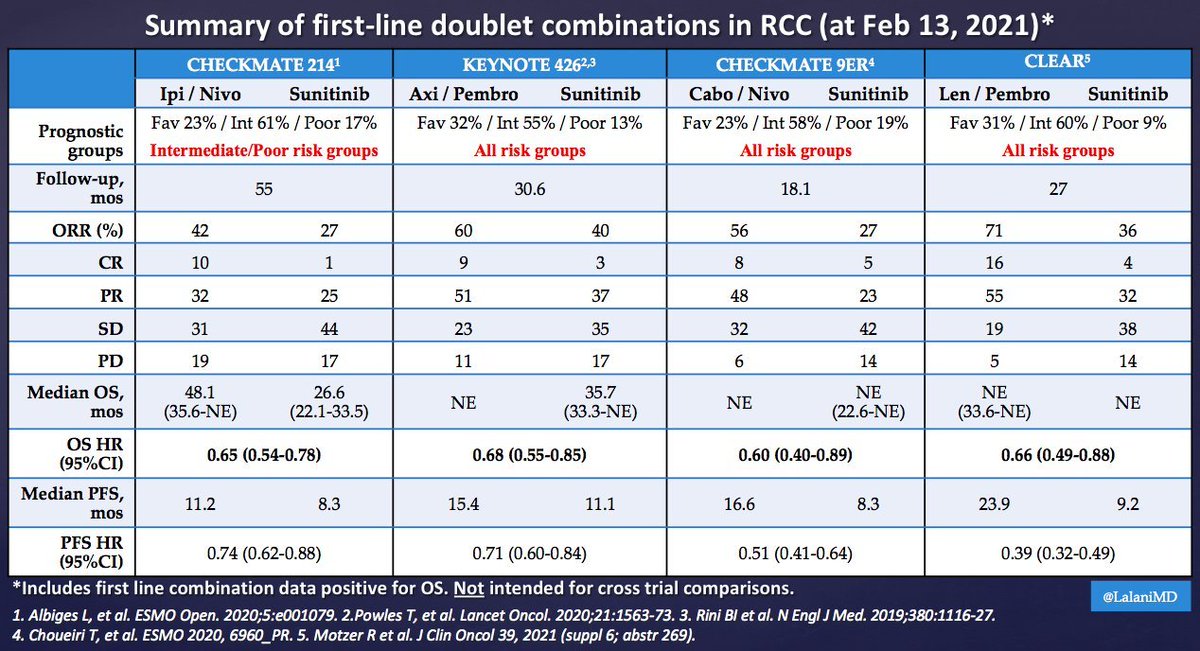
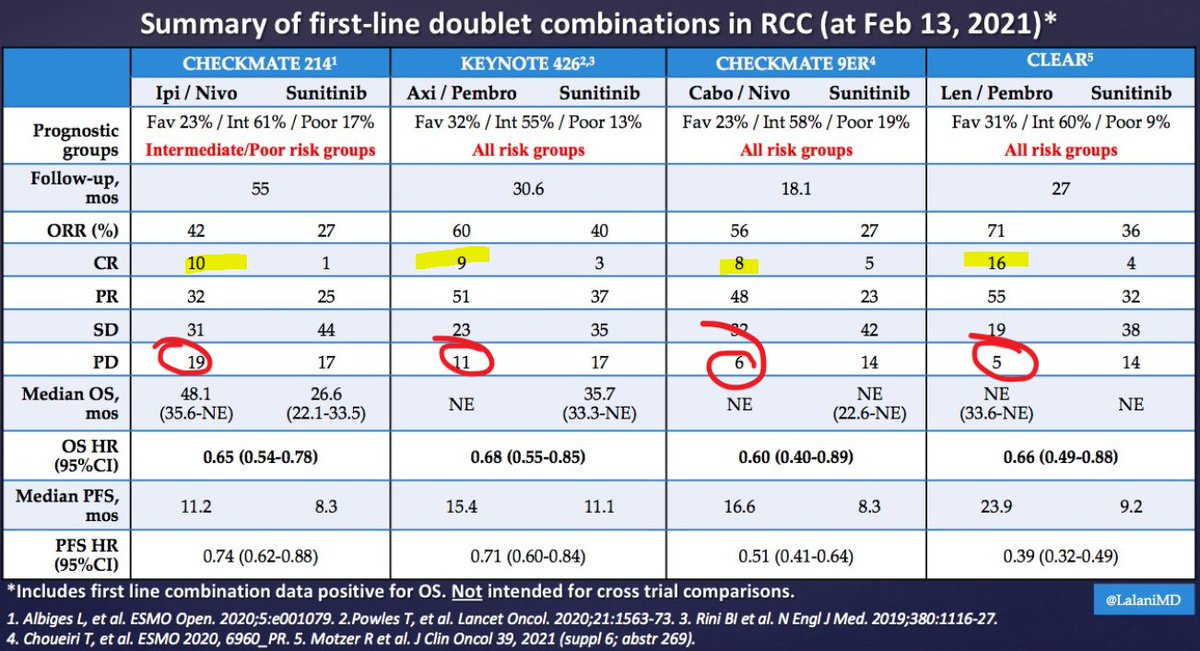
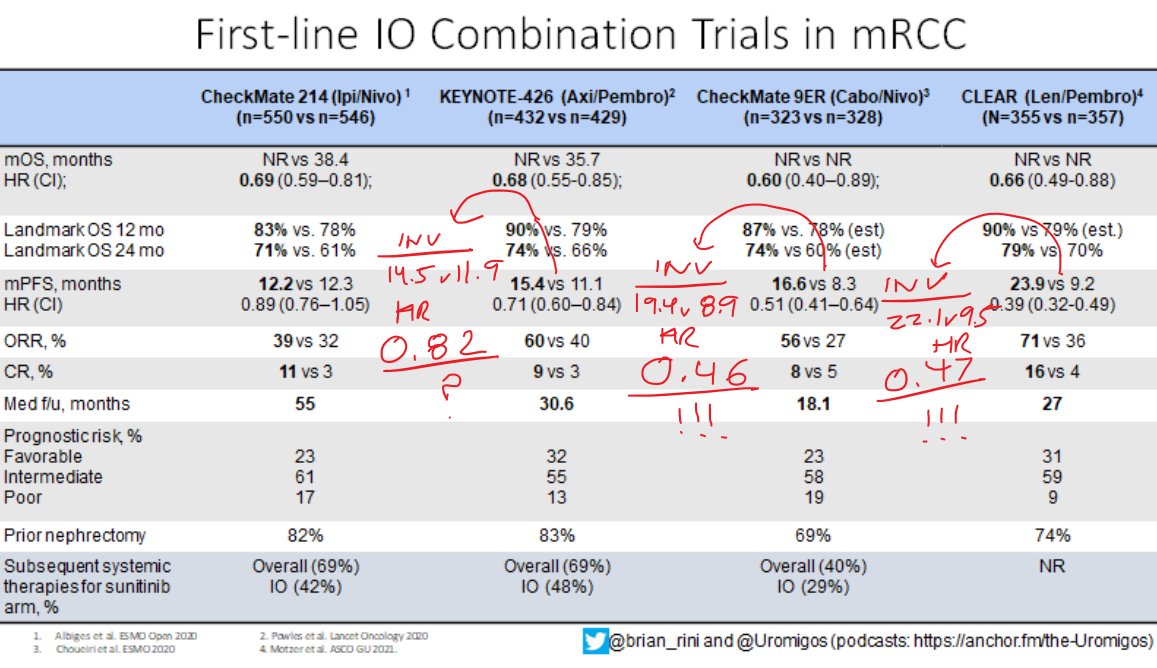
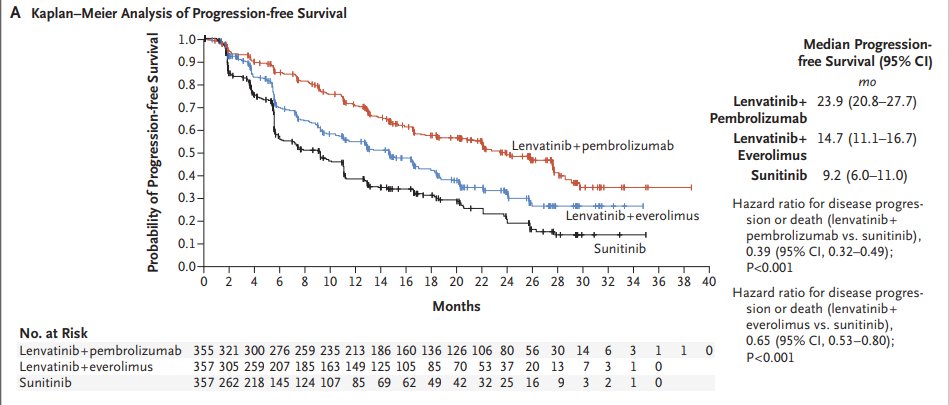
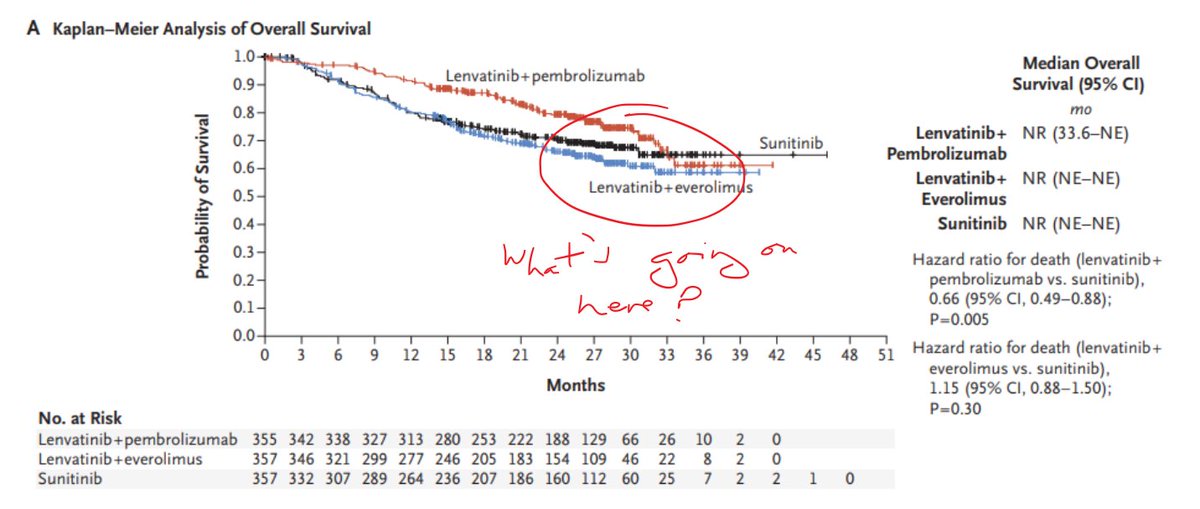
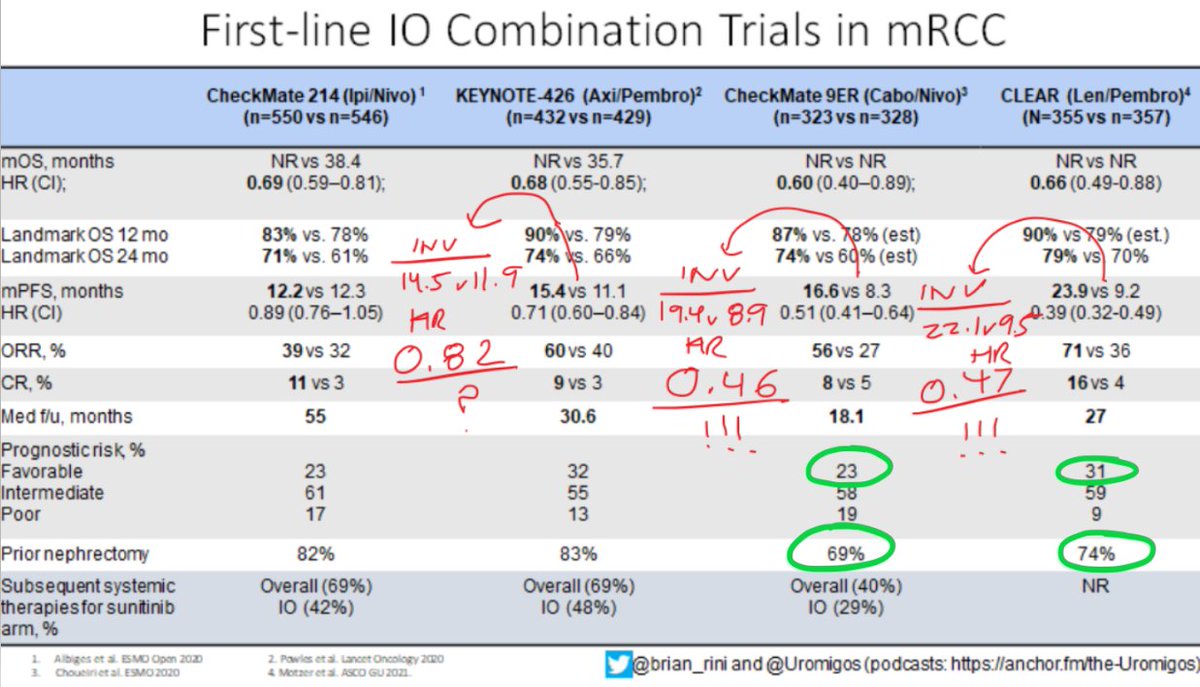
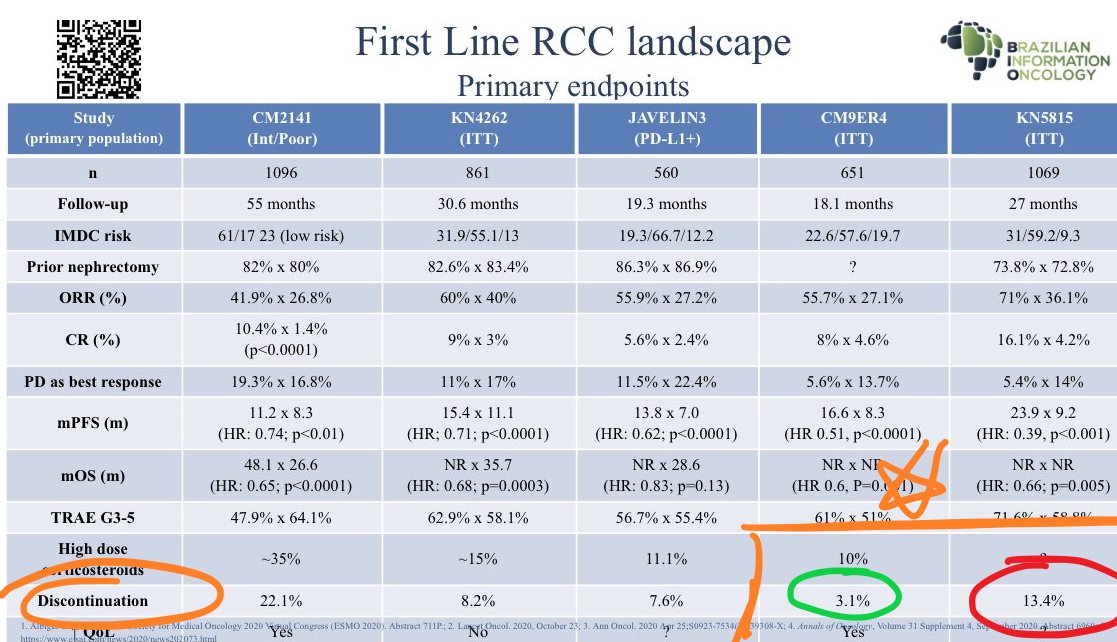
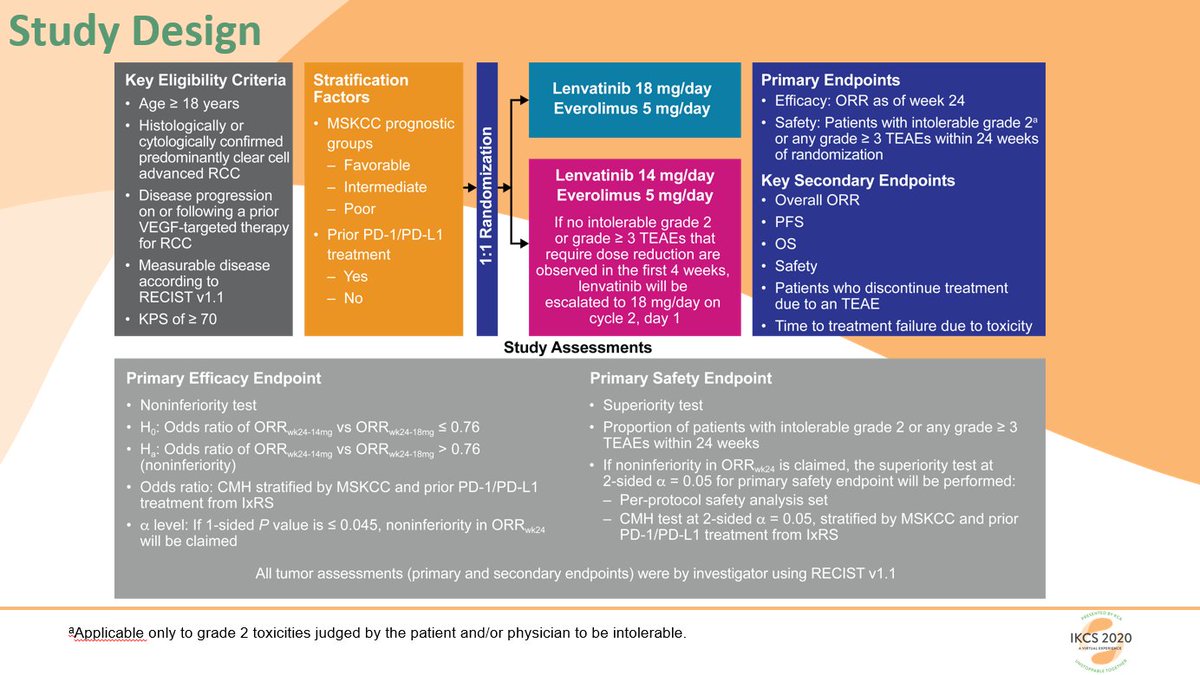
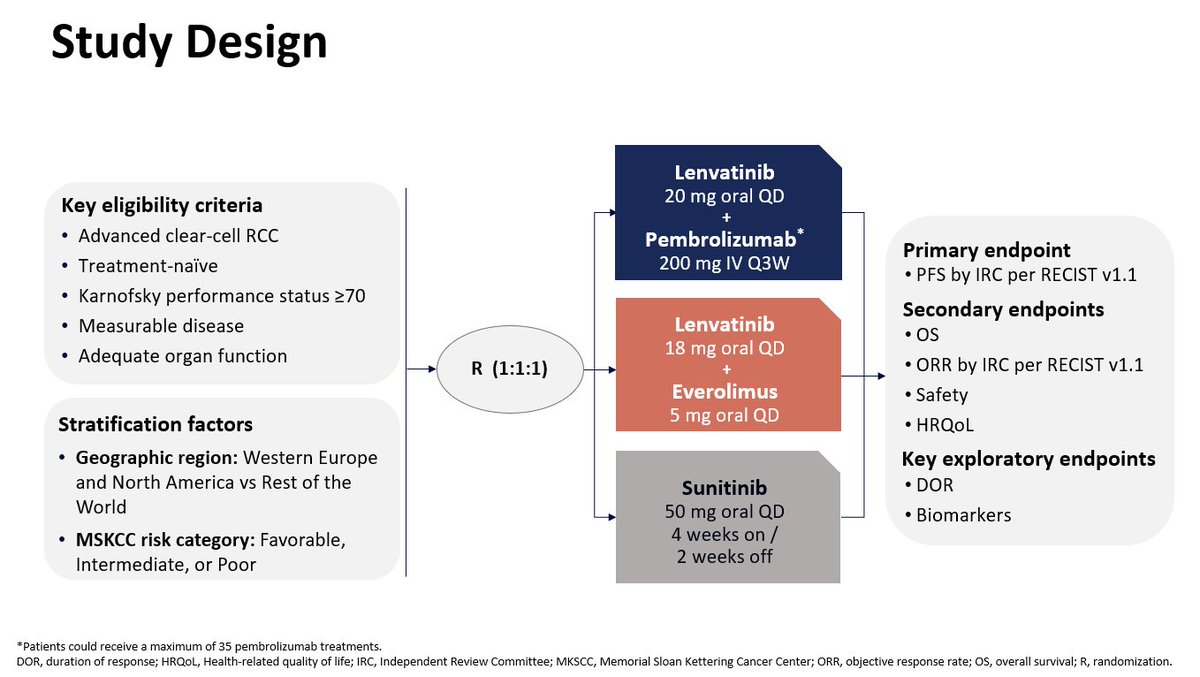
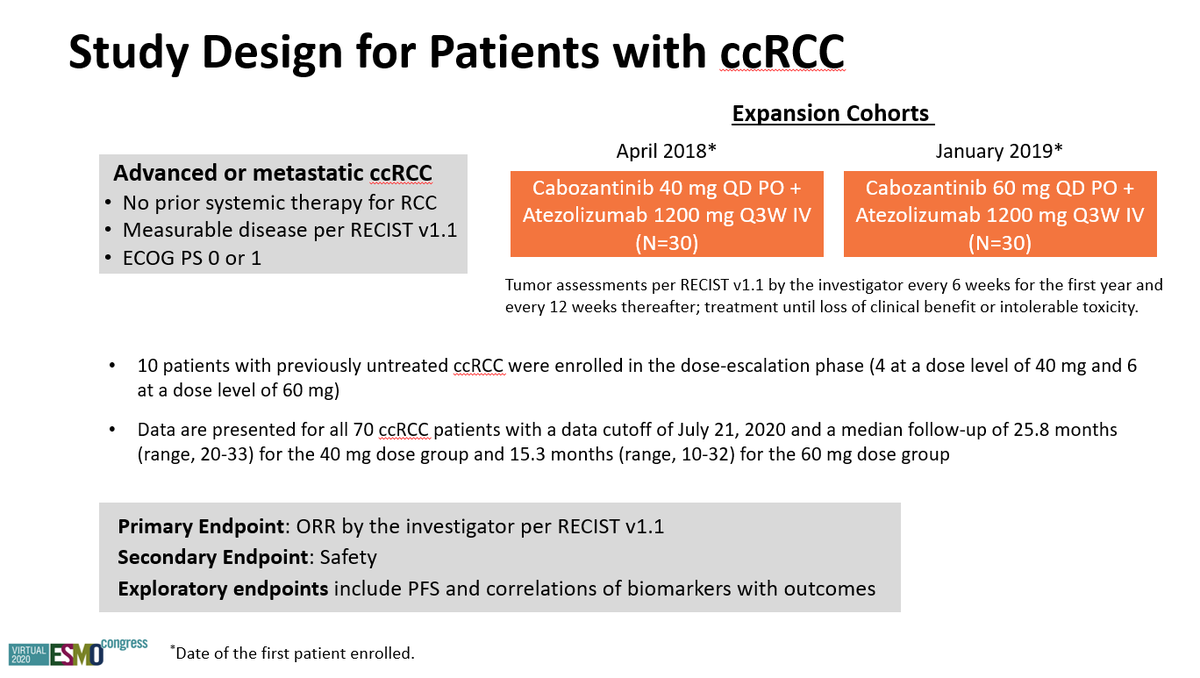
It's Monday AM post-@ASCO #GU21 & clinic starts in a couple of hours! Lots to process - I'll try to tackle optimal 1L tx for #kidneycancer. I'll make a case for cabo/nivo, leaning on the beautiful (& timely) tables below from @lalaniMD, @SoaresAndrey & @brian_rini (1/15)

More from Health

You gotta think about this one carefully!
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
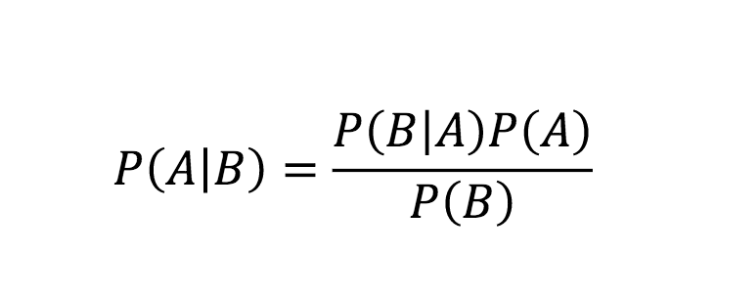
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
Really doesn\u2019t fit well in a tweet. pic.twitter.com/xN0pAyniFS
— Dr. Lena Sugar \U0001f3f3\ufe0f\u200d\U0001f308\U0001f1ea\U0001f1fa\U0001f1ef\U0001f1f5 (@_jvs) February 18, 2021
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇





Now you know I love to sh-t in Harvard. But I also like accuracy. So I decided to go look at Harvard’s catalog to see its lack of military history that this article describes (they only teach history of pets it claims) and what I found shocked me! Shocked me! A thread: 1/
First off, Harvard students literally have multiple sections of military history that they can take listed. (It appears these ones are taught at MIT, so they might have to walk down the street for these) but... 2/

Say they want to stay on campus...they can only take numerous classes on war and diplomacy...3/
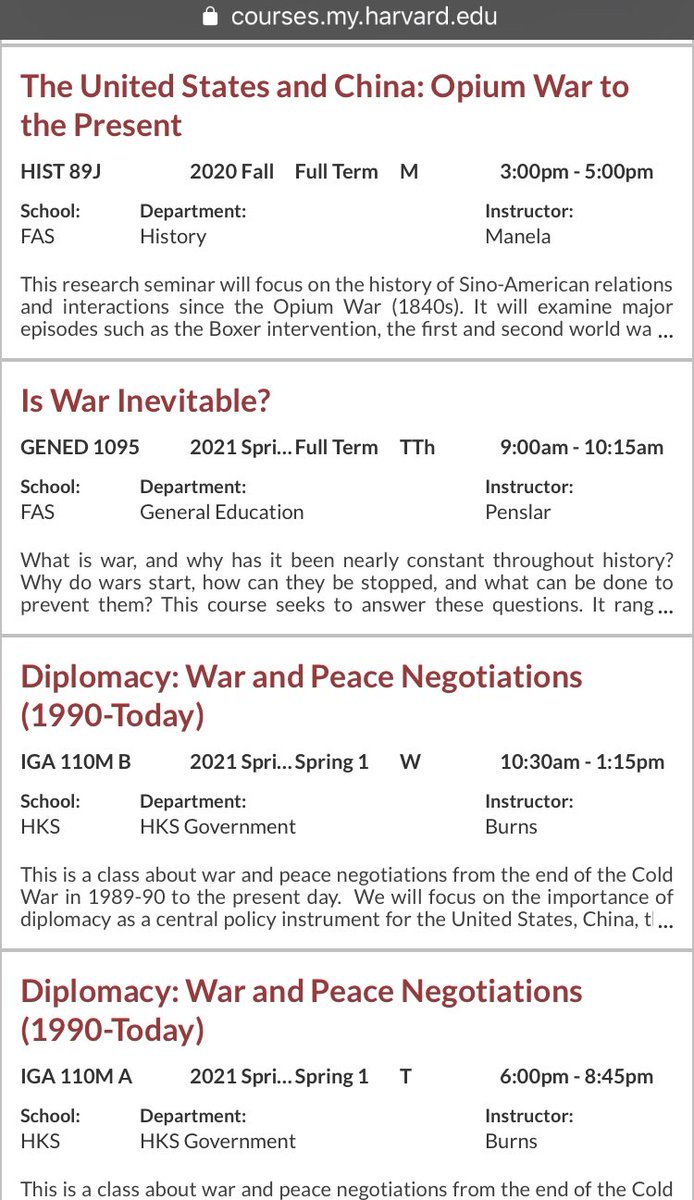
They have an entire class on Yalta. That’s right. An entire class on Yalta. 4/

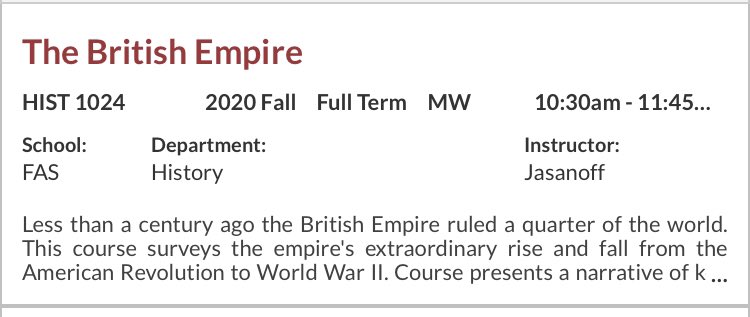
But wait! There is more! They can take the British Empire, The Fall of the Roman Empire for those wanting traditional topics... 5/
\u201cMilitary history\u201d is only in decline if you\u2014like the author & experts in this obnoxious piece\u2014see the subject as a narrowly defined, white dude-oriented, guns & bayonets approach. The field is 1000% better off w/today\u2019s diversity of topics & historians. https://t.co/dUf3OWyVpQ
— Jonathan S. Jones (@_jonathansjones) February 1, 2021
First off, Harvard students literally have multiple sections of military history that they can take listed. (It appears these ones are taught at MIT, so they might have to walk down the street for these) but... 2/
Say they want to stay on campus...they can only take numerous classes on war and diplomacy...3/
They have an entire class on Yalta. That’s right. An entire class on Yalta. 4/
But wait! There is more! They can take the British Empire, The Fall of the Roman Empire for those wanting traditional topics... 5/