What about IO/IO? We have long f/u w #CM214 data w nivo/ipi, no doubt (@AlbigesL et al in
@myESMO Open). And treatment-free interval discussed by McDermott
@BIDMChealth is no doubt impt. But we've known data not as impressive for favorable risk (2/15)
And furthermore, as
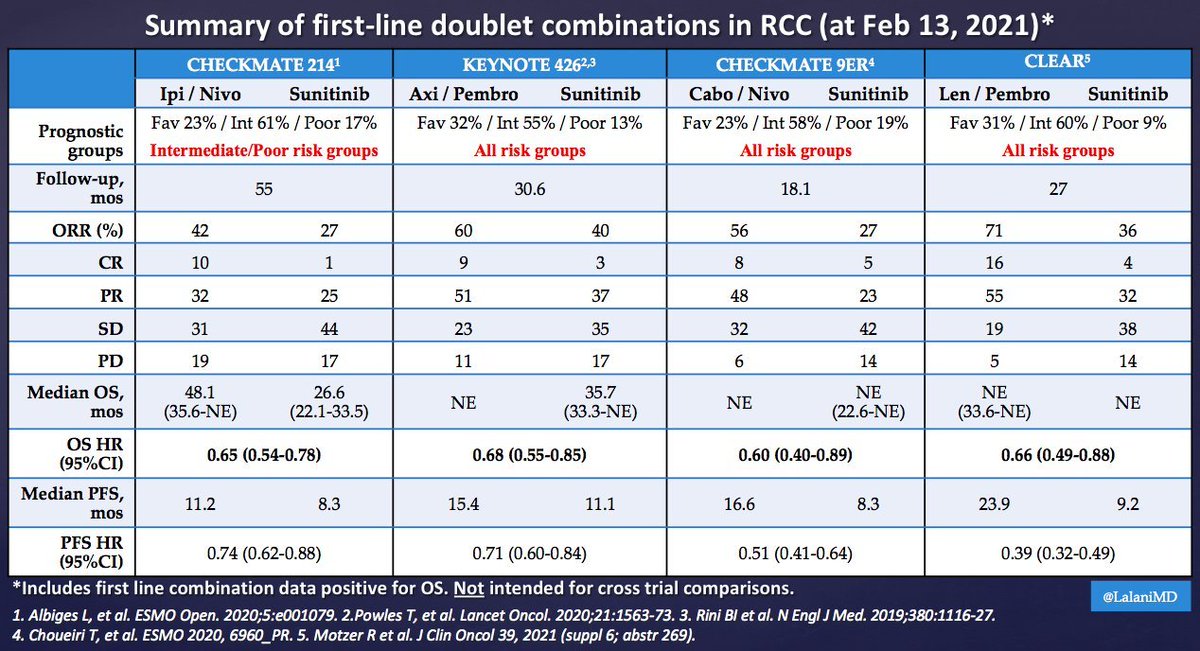
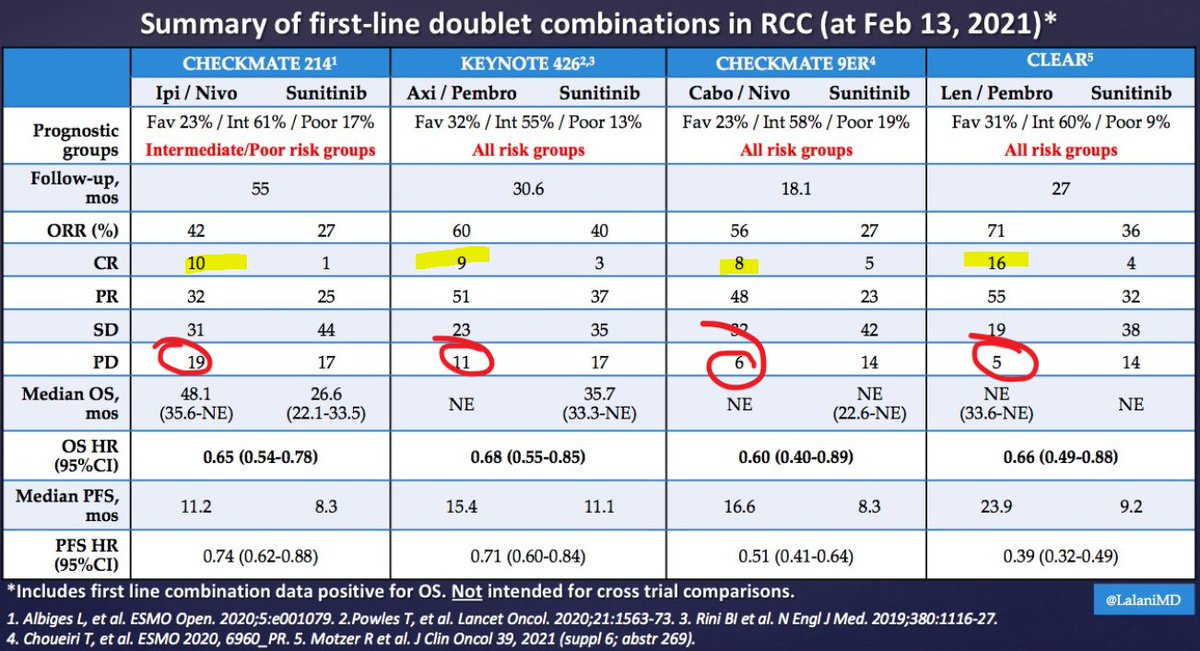
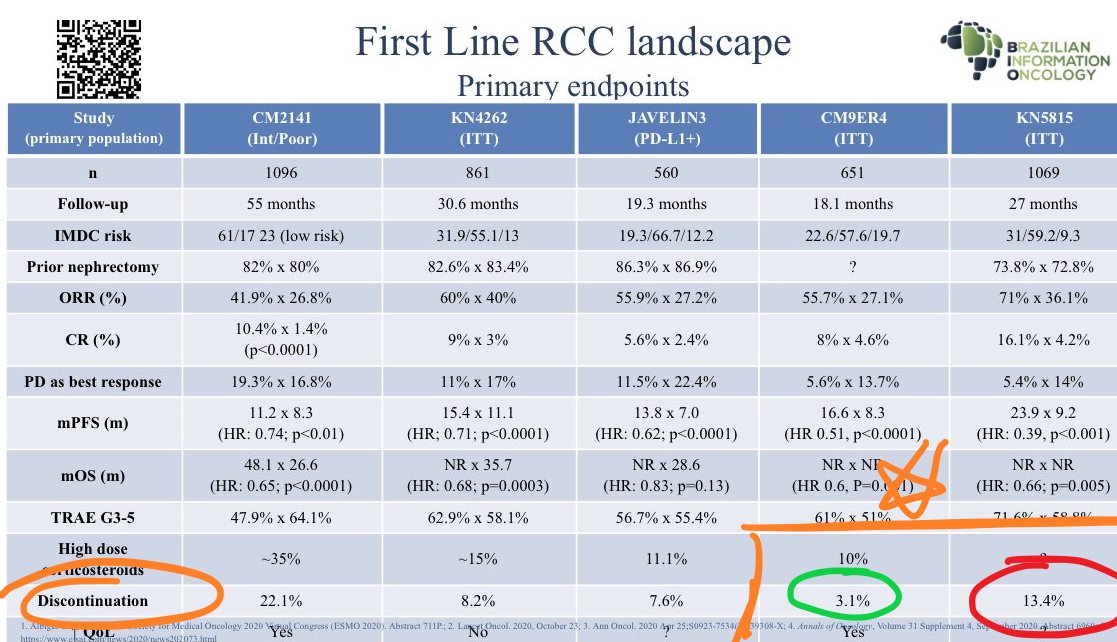
@ERPlimackMD points out in another tweet, impt to look at primary PD rates (seen in
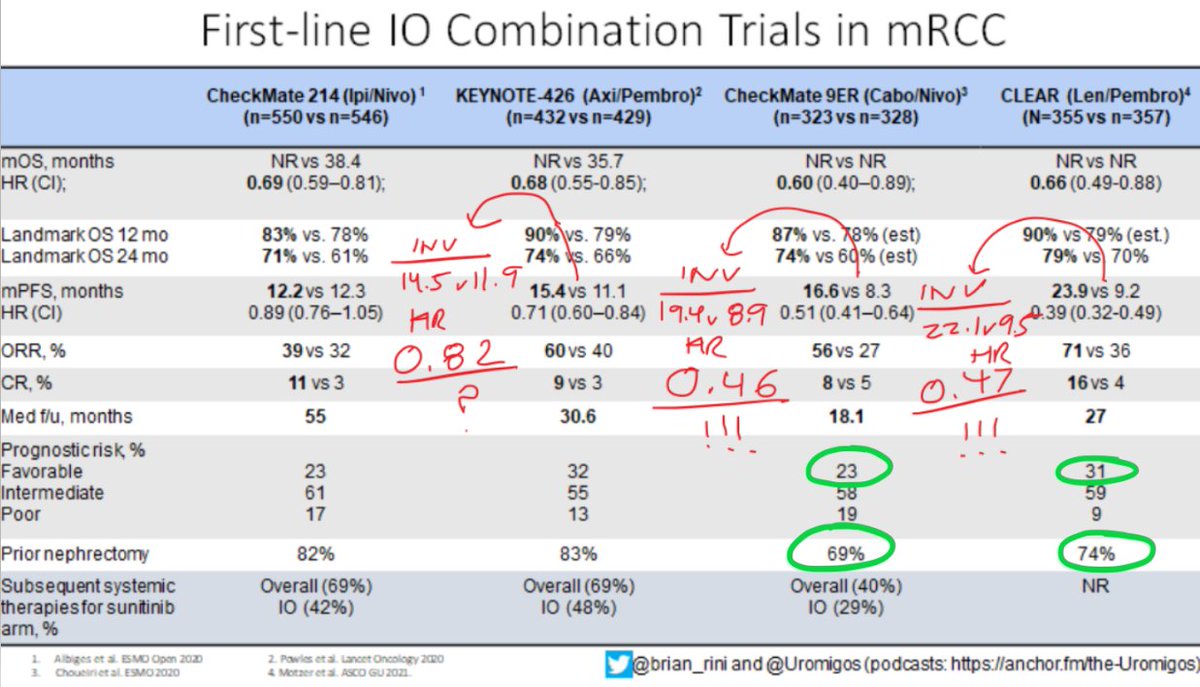
@lalaniMD's table) - nivo/ipi at 19%!!! CR rate used to be something we highlighted w nivo/ipi, but now comparable across studies (3/15)
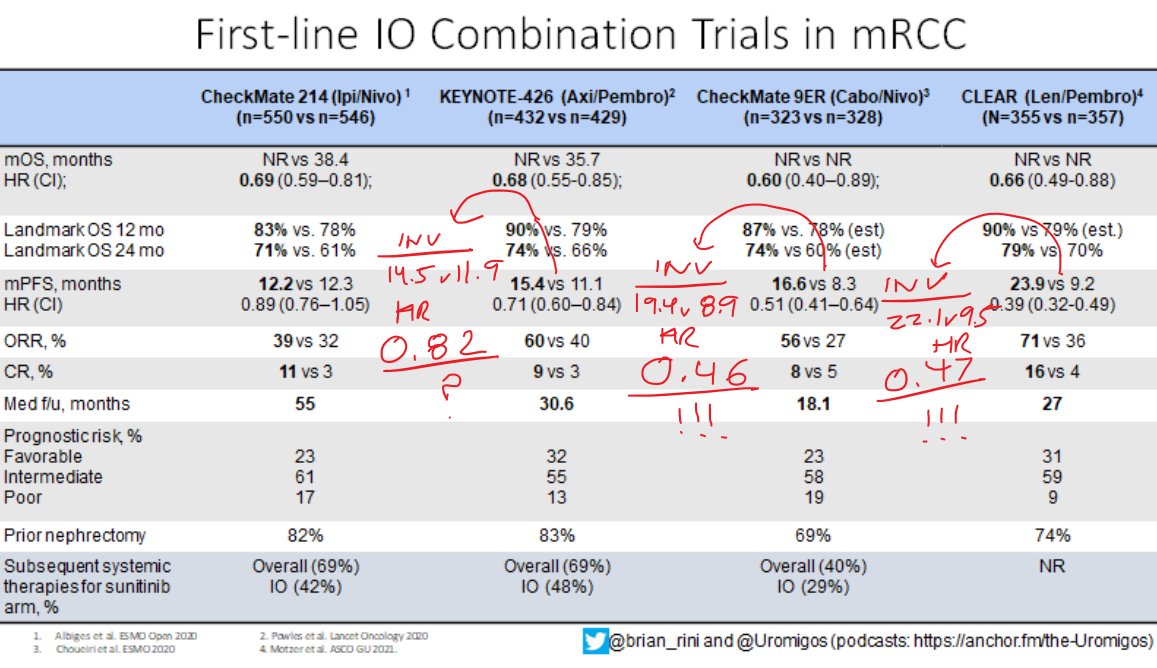
Okay now to the really tough stuff - comparing TKI/IO regimens. Something interesting I will add to
@brian_rini @uromigos table above is the HR for PFS by INVESTIGATOR review. If the diff in HR for PFS by IND review caught your eye, this is even more striking (4/15)
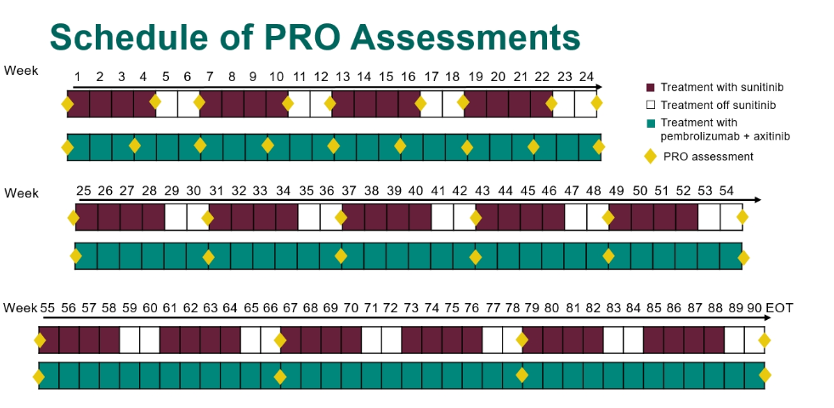
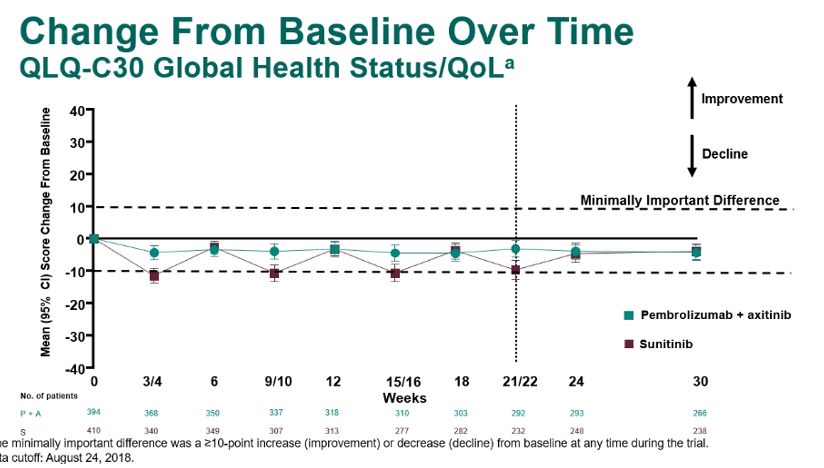
I think INV-assessed PFS is impt, but if you're a skeptic, forget that argument. Turn instead to #QOL with axi/pembro. Kudos to
@brian_rini @tompowles1 @ERPlimackMD et al for advocating for QOL in KN-426.
@crisbergerot et al have taughts us the importance of these metrics. (5/15)
Unfortunately, we're not seeing any improvement in QOL w axi/pembro. This is a bit concerning - if balanced between arms, are we prolonging PFS at the expense of the patient's overall well-being? Inc tumor regression should be accompanied by some symptomatic improvement. (6/15)
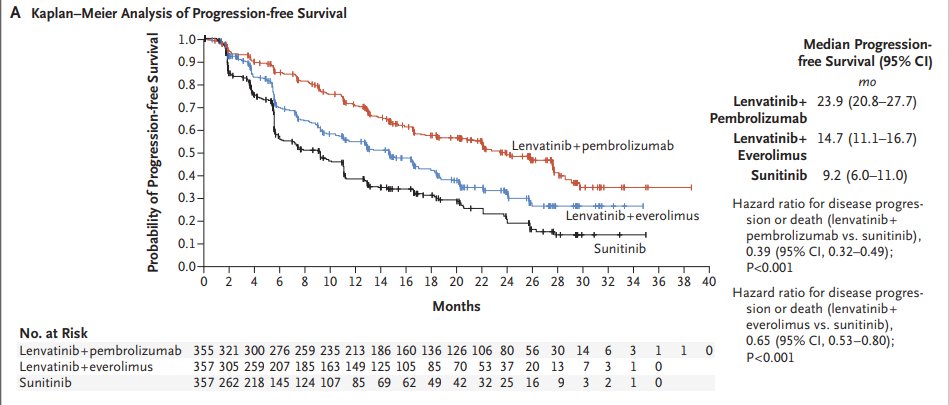
Okay, now on to one of the headliners at
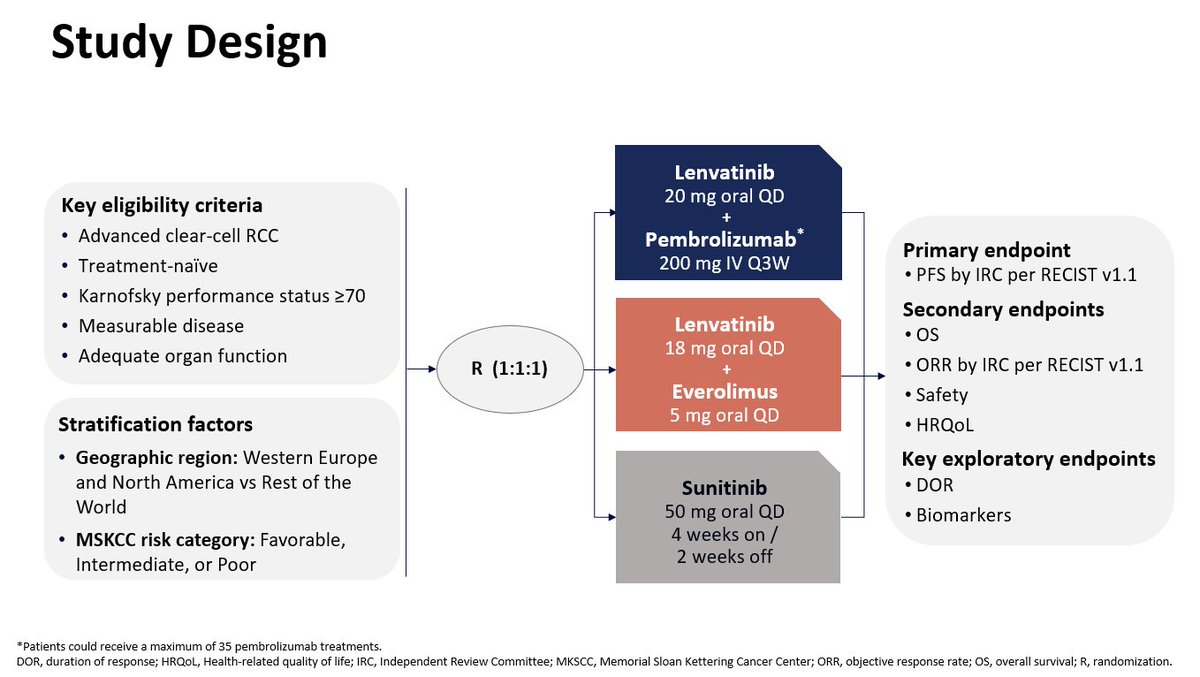
@ASCO #GU21 this past weekend. The CLEAR study presented by
@motzermd @DrChoueiri @DrTHut @tompowles1 @CPRT65 et al. Simultaneously published in
@NEJM - congrats friends! (7/15)
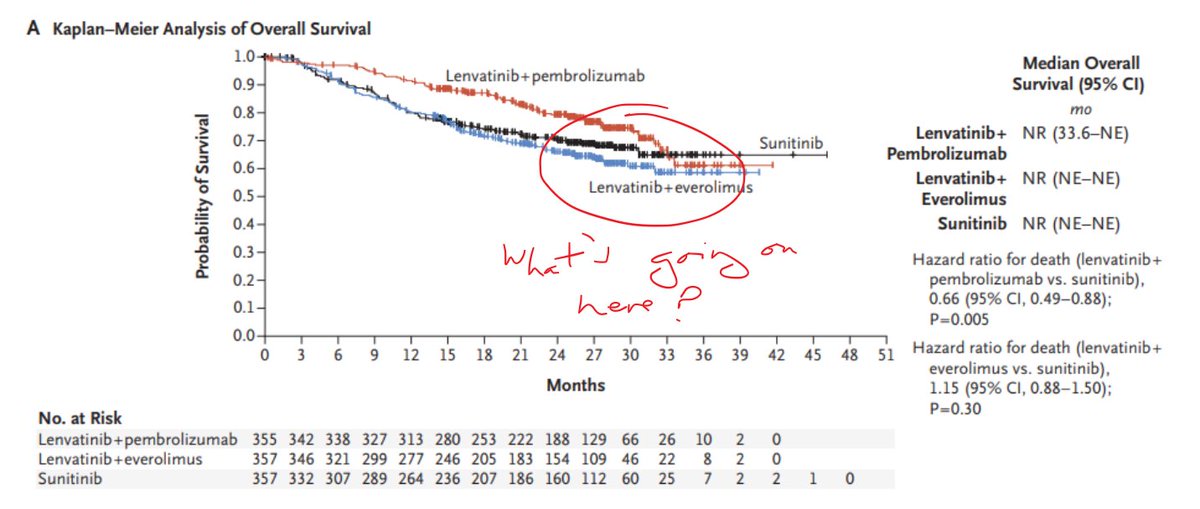
Just one point on the curves, which I heard
@tompowles1 bring up on a
@Uromigos podcast w
@DrChoueiri (of note, I also saw
@manuelmaiamd bring this up during
@motzermd's presentation in the
@ASCO #GU21 pres). Why do the OS curves merge? Not so in #CheckMate9ER! (8/15)
Regardless, some may be swayed by the 16% CR rate with len/pembro. Now HERE is where we need to dive into baseline characteristics. Nearly 10% more fav risk in CLEAR, and also, more pts with prior neph. So, the odds of getting CR (or even PR) stacked against #CheckMate9ER (9/15)
I'll next make the point that LEN IS HARD TO TOLERATE. I'm glad
@SoaresAndrey highlights the rate of discontinuation in #CLEAR, which appears much higher than in #CheckMate9ER. I've seen 7al versions of the data, but no matter how you slice it, d/c rate⬆️with len/pembro. (10/15)
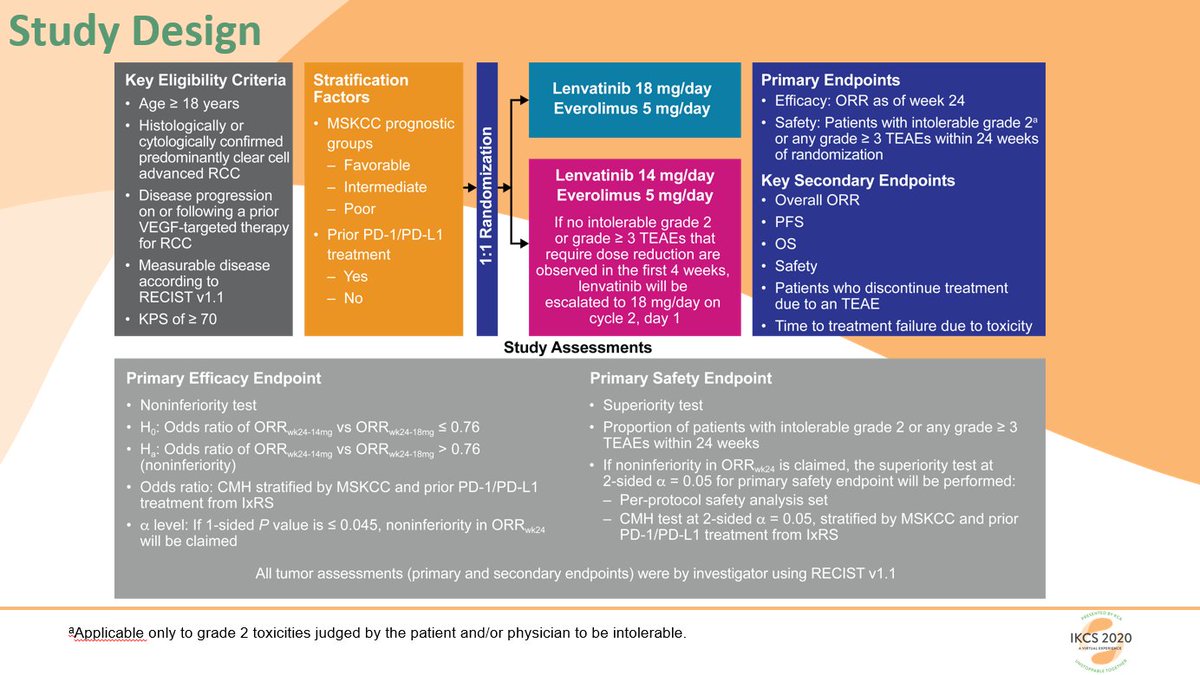
What's my experience with len? I ran a RP2 study w
@DrDanielHeng @hipsytips @docjavip et al. We tried to lower dose from 18 to 14 mg & preserve efficacy, but with the caveat of this being a small non-inferiority study, it didn't appear feasible. 👀rates of d/c due to AEs! (11/15)
Remember, I was comparing 18 and 14 mg. The dose in #CLEAR even HIGHER at 20 mg! This is one of those settings where QOL data ESSENTIAL. Remember, our pts are thankfully doing better & will be on drug longer - we need to look out for their GLOBAL well-being! (12/15)
Now THIS is what we need to see. Improved QOL with cabo/nivo, as
@DrChoueiri presented at #ESMO20. Remember, the dose of 40 mg is used in #CheckMate9ER - LOWER than the dose of 60 mg used in #METEOR, with cabo as 2L/3L tx. (13/15).
Confession: I was skeptical when
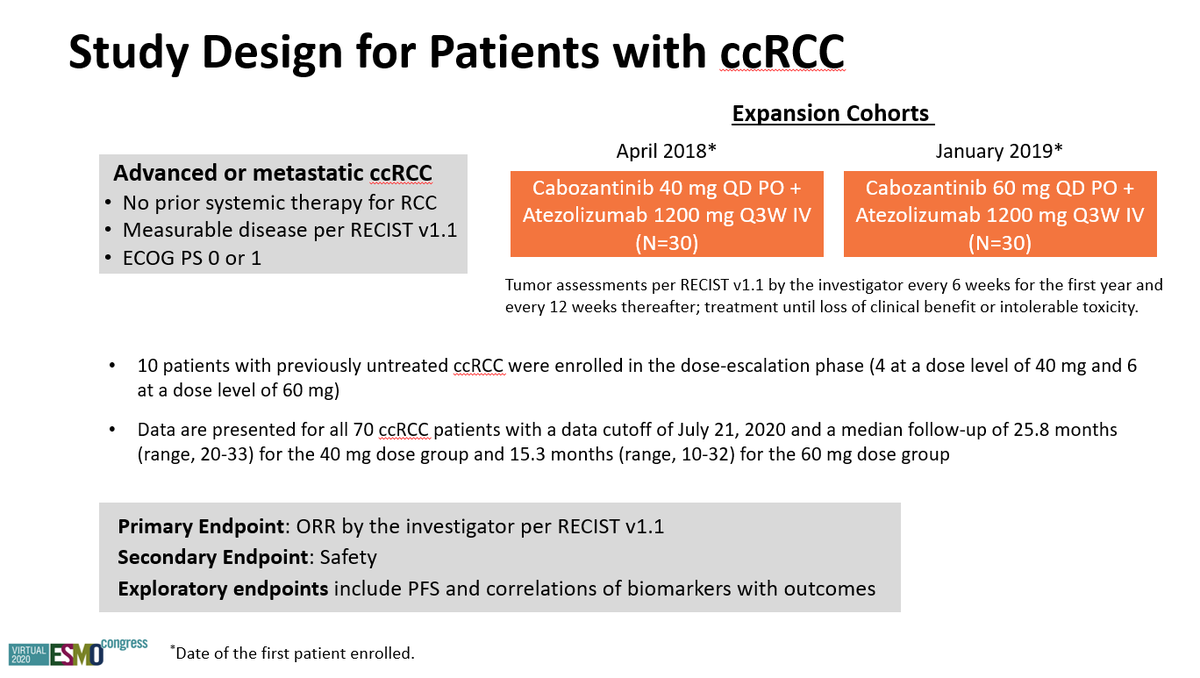
@DrChoueiri @motzermd @tompowles1 @apolo_andrea & the brilliant team for #CheckMate9ER chose 40. But
@neerajaiims & I have since reported data from #COSMIC021 (cabo/atezo across multiple settings). Efficacy at both doses seems quite good (14/15)
SUMMARY: In 2021, we are blessed w gr8 data from mult 1L trials in #kidneycancer. I feel that cabo/nivo is the way to go; the goalpost is shifted beyond just PFS/RR/OS, we now need QOL! Thx to the amazing data summaries that facilitated this thread. Open to all comments. (15/15)