

Folks, we need to talk about this Vitamin D trial. I have no stake in this game - take Vitamin D if you want but this pre-print is super sus.



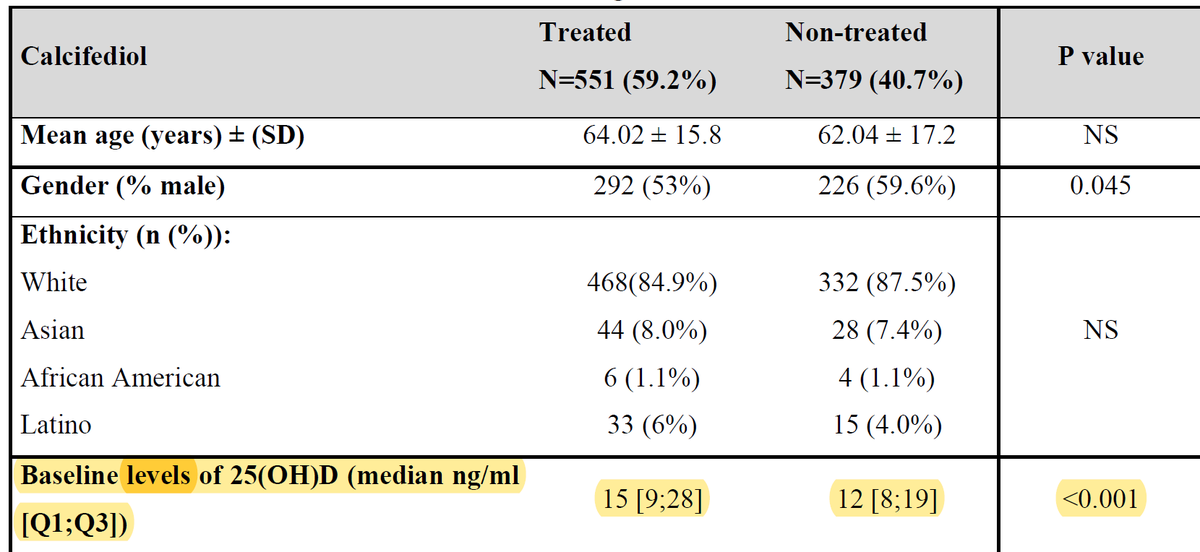
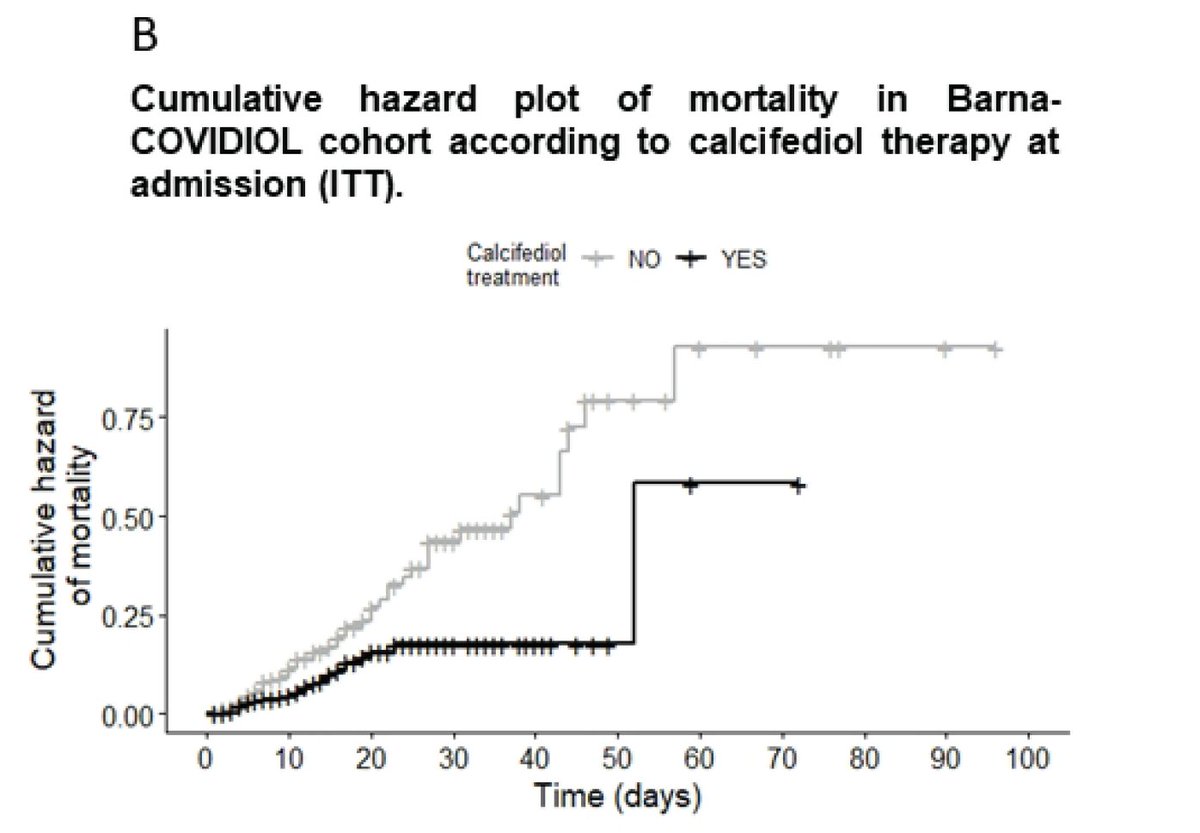
https://t.co/XVmsiajpBr
Trust me- vitamin D > vaccine . @foundmyfitness been preaching this from the start. 4000 iu daily \u203c\ufe0f\u203c\ufe0f https://t.co/2oSgJ3KdwB
— Harry Grant (@Harrygrant123) February 14, 2021
More from Health








Some thoughts on this: Firstly, it might be personal preference, but I am not keen on this kind of campaign as I feel like it trivialises cancer. Sometimes the serious message gets lost because people are sharing pics of cats or whatever and the important context is gone.
More importantly, the statistic being used in the campaign is misleading. It says 57% of women put off cervical screening if they can't get waxed. But on further investigation, that's not accurate.
The page here goes on to say "57% of women who regularly have their pubic hair professionally removed would put off attending their cervical screening appointment if they hadn’t been able to visit a beauty salon."
So the 57% represents a concern not across the whole population of women, but only those who regularly get waxed. So how big of an issue is this across the whole population? And what else is stopping people getting smears?
I think campaigns for cancer screening are really tricky because there is so much nuance that often doesn't fit into a catchy headline or hashtag. It's certainly not easy and is part of a bigger conversation.
It\u2019s #CervicalCancerPreventionWeek \U0001f499
— myGP (@myGPapp) January 18, 2021
Here\u2019s how you can help to raise awareness:
\U0001f431 Share an image of the cat that best reflects your undercarriage/flower/bits (technical term vulva!) current look.
#\u20e3Use the Hashtag #myCat.
\U0001f46dTell and tag your friends to let them know. pic.twitter.com/8aHf96ynjT
More importantly, the statistic being used in the campaign is misleading. It says 57% of women put off cervical screening if they can't get waxed. But on further investigation, that's not accurate.
The page here goes on to say "57% of women who regularly have their pubic hair professionally removed would put off attending their cervical screening appointment if they hadn’t been able to visit a beauty salon."
So the 57% represents a concern not across the whole population of women, but only those who regularly get waxed. So how big of an issue is this across the whole population? And what else is stopping people getting smears?
I think campaigns for cancer screening are really tricky because there is so much nuance that often doesn't fit into a catchy headline or hashtag. It's certainly not easy and is part of a bigger conversation.

Thread on how atheism leads to mental retardation (backed with medical citations🧵💉)
To start with, atheism is an unnatural self-contradicting doctrine.
Medical terminology proves that human beings are naturally pre-disposed to believe in God. Oxford scientists assert that people are "born believers".
https://t.co/kE0Fi588yn
https://t.co/OqyXcGIMJn

It should be known that atheism could never produce an intelligently-functioning society and neither ever will.
Contrastingly, Islam produced several intellectuals & polymaths, was on the forefront of scientific development, boasting 100% literacy
It is also scientifically proven that atheism led to lesser scientific curiosity and scientific frauds, which is also why atheists incline to pseudo-science.
Whereas, religion in general and Islam in particular boosted education.
https://t.co/19Onc84u3g

Atheists are also likely to affected by pervasive mental and developmental disorders like high-functioning autism.
Cognitive Scientists and renowned Neurologists found that more atheism is leads to greater autism.
https://t.co/zRjEyFoX3P

To start with, atheism is an unnatural self-contradicting doctrine.
Medical terminology proves that human beings are naturally pre-disposed to believe in God. Oxford scientists assert that people are "born believers".
https://t.co/kE0Fi588yn
https://t.co/OqyXcGIMJn
It should be known that atheism could never produce an intelligently-functioning society and neither ever will.
Contrastingly, Islam produced several intellectuals & polymaths, was on the forefront of scientific development, boasting 100% literacy
If the Muslim world had not existed, there literally would be no technology/achievements today.
— Starks\u262a\ufe0f\U0001f1f9\U0001f1e9 (@MegaIntelIect) January 8, 2021
Science only developed because of Islam, Europe should be grateful to Islam for civilizing their barbaric cult.
Source: The Caliph's Splendor, Pg 204-05 https://t.co/HVypO52Tpc pic.twitter.com/00jYSbaDSs
It is also scientifically proven that atheism led to lesser scientific curiosity and scientific frauds, which is also why atheists incline to pseudo-science.
Whereas, religion in general and Islam in particular boosted education.
https://t.co/19Onc84u3g
Atheists are also likely to affected by pervasive mental and developmental disorders like high-functioning autism.
Cognitive Scientists and renowned Neurologists found that more atheism is leads to greater autism.
https://t.co/zRjEyFoX3P
You May Also Like







fascinated by this man, mario cortellucci, and his outsized influence on ontario and GTA politics. cortellucci, who lives in vaughan and ran as a far-right candidate for the italian senate back in 2018 - is a major ford donor...

his name might sound familiar because the new cortellucci vaughan hospital at mackenzie health, the one doug ford has been touting lately as a covid-centric facility, is named after him and his family
but his name also pops up in a LOT of other ford projects. for instance - he controls the long term lease on big parts of toronto's portlands... where doug ford once proposed building an nfl stadium and monorail... https://t.co/weOMJ51bVF
cortellucci, who is a developer, also owns a large chunk of the greenbelt. doug ford's desire to develop the greenbelt has been
and late last year he rolled back the mandate of conservation authorities there, prompting the resignations of several members of the greenbelt advisory
his name might sound familiar because the new cortellucci vaughan hospital at mackenzie health, the one doug ford has been touting lately as a covid-centric facility, is named after him and his family
but his name also pops up in a LOT of other ford projects. for instance - he controls the long term lease on big parts of toronto's portlands... where doug ford once proposed building an nfl stadium and monorail... https://t.co/weOMJ51bVF
cortellucci, who is a developer, also owns a large chunk of the greenbelt. doug ford's desire to develop the greenbelt has been
and late last year he rolled back the mandate of conservation authorities there, prompting the resignations of several members of the greenbelt advisory



1/OK, data mystery time.
This New York Times feature shows China with a Gini Index of less than 30, which would make it more equal than Canada, France, or the Netherlands. https://t.co/g3Sv6DZTDE
That's weird. Income inequality in China is legendary.
Let's check this number.
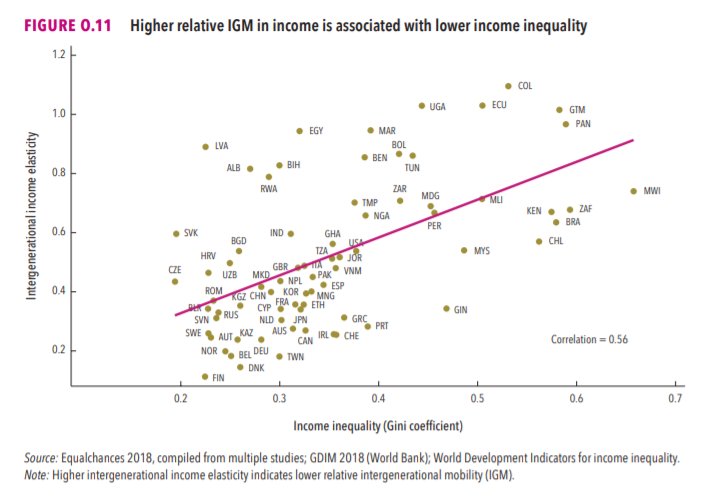
2/The New York Times cites the World Bank's recent report, "Fair Progress? Economic Mobility across Generations Around the World".
The report is available here:
3/The World Bank report has a graph in which it appears to show the same value for China's Gini - under 0.3.
The graph cites the World Development Indicators as its source for the income inequality data.
4/The World Development Indicators are available at the World Bank's website.
Here's the Gini index: https://t.co/MvylQzpX6A
It looks as if the latest estimate for China's Gini is 42.2.
That estimate is from 2012.
5/A Gini of 42.2 would put China in the same neighborhood as the U.S., whose Gini was estimated at 41 in 2013.
I can't find the <30 number anywhere. The only other estimate in the tables for China is from 2008, when it was estimated at 42.8.
This New York Times feature shows China with a Gini Index of less than 30, which would make it more equal than Canada, France, or the Netherlands. https://t.co/g3Sv6DZTDE
That's weird. Income inequality in China is legendary.
Let's check this number.
2/The New York Times cites the World Bank's recent report, "Fair Progress? Economic Mobility across Generations Around the World".
The report is available here:
3/The World Bank report has a graph in which it appears to show the same value for China's Gini - under 0.3.
The graph cites the World Development Indicators as its source for the income inequality data.
4/The World Development Indicators are available at the World Bank's website.
Here's the Gini index: https://t.co/MvylQzpX6A
It looks as if the latest estimate for China's Gini is 42.2.
That estimate is from 2012.
5/A Gini of 42.2 would put China in the same neighborhood as the U.S., whose Gini was estimated at 41 in 2013.
I can't find the <30 number anywhere. The only other estimate in the tables for China is from 2008, when it was estimated at 42.8.
