
1/ An excellent new paper from Denmark that tracks every vaccination given to nursing home residents there shows an 40% RISE in infections immediately after the first @pfizer dose and no efficacy at any point. Protection in this population after “full” vaccination is 64%...
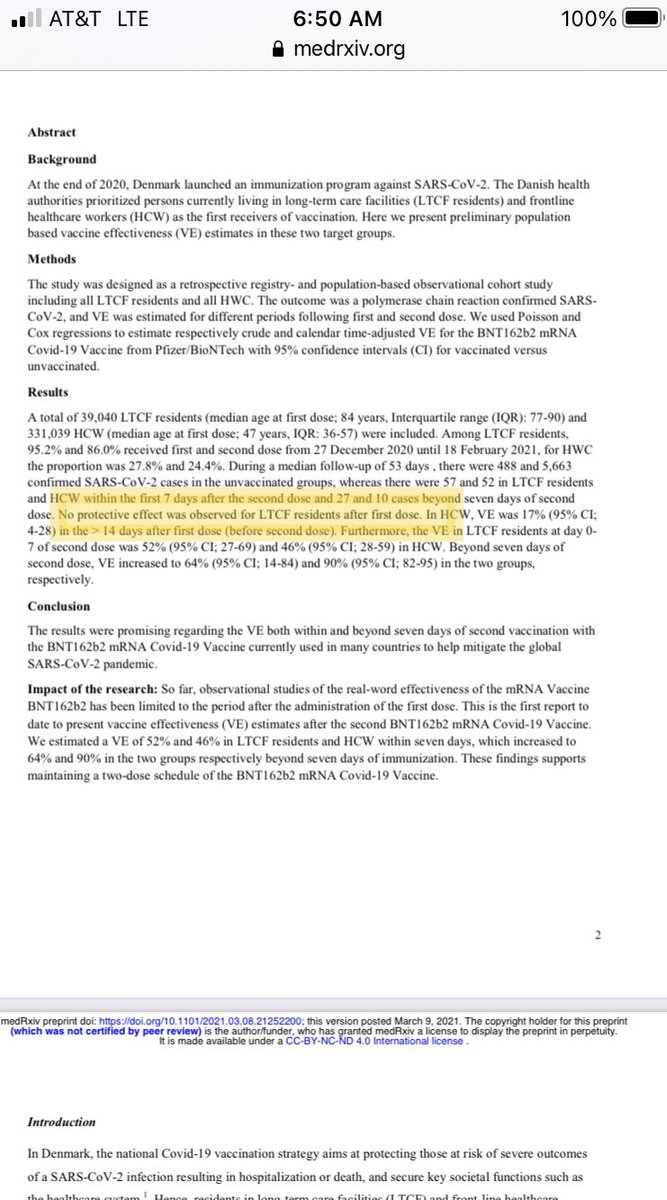
Source: https://t.co/RtyNiWlfXL
More from Category c19




1/ Thread – THE YEAR OF THE RAT
“15 days to slow the spread” began one year ago. It was March 2020, the Year of the Rat. Never was any year more fitting of the name. Never in history have the people been betrayed so callously, flagrantly and absolutely by their alleged leaders.

2/ They were betrayed by their WHO
3/ and their national health
4/ They were betrayed by medical
5/ and their peer
“15 days to slow the spread” began one year ago. It was March 2020, the Year of the Rat. Never was any year more fitting of the name. Never in history have the people been betrayed so callously, flagrantly and absolutely by their alleged leaders.
2/ They were betrayed by their WHO
3/ and their national health
4/ They were betrayed by medical
Despite ignorance by many in the West, this article by The Lancet is a powerful endorsement of China\u2019s successful pandemic response. Hate to read stories by those paparazzi journalists who are experts at spinning but have little knowledge of science. https://t.co/Q8rKwwTPsI pic.twitter.com/436BEmx9nl
— Chen Weihua \uff08\u9648\u536b\u534e\uff09 (@chenweihua) October 16, 2020
5/ and their peer
6/ Eurosurveillance, a journal whose editors coincidentally includes Mr. Drosten, takes only a single day for the peer review process and publishes the hastily compiled PCR protocol on January 22. https://t.co/cWX3UdKeID
— Pace \U0001f642 (@theotherphilipp) February 25, 2021

All you need to know about COVID19
FACTS NOT FEAR
Covid 19 is a disease caused by the SARS-CoV-2 virus. SARS-CoV-2 is one of 7 coronaviruses known to man. 1/n
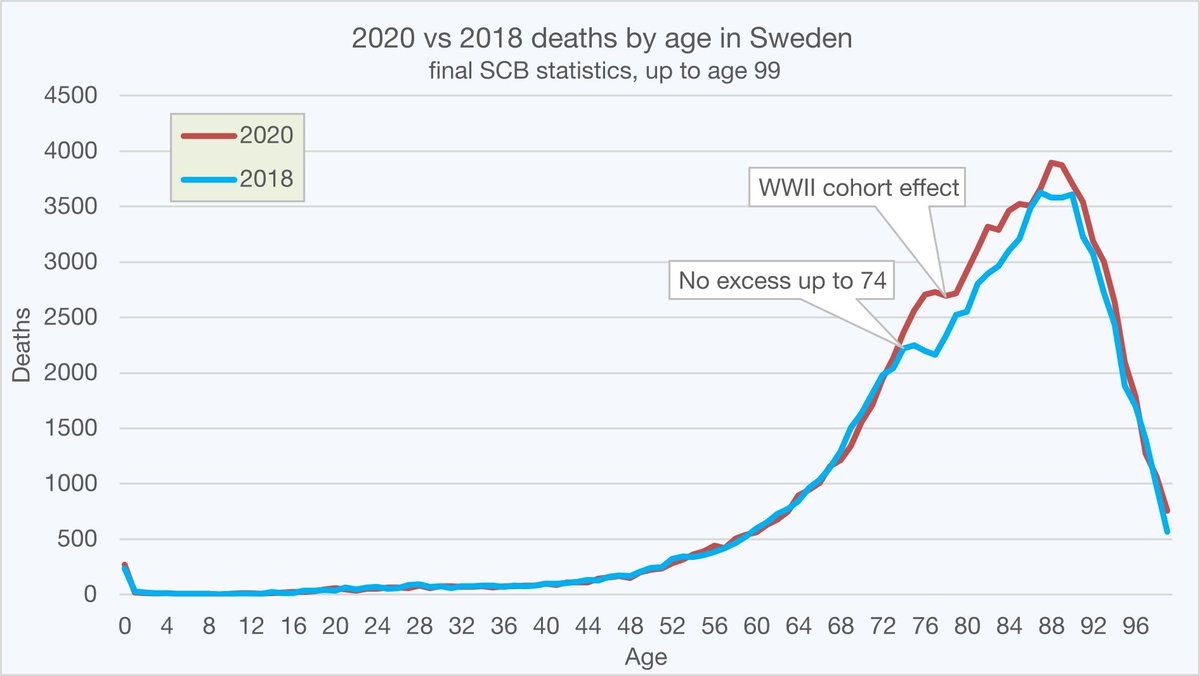
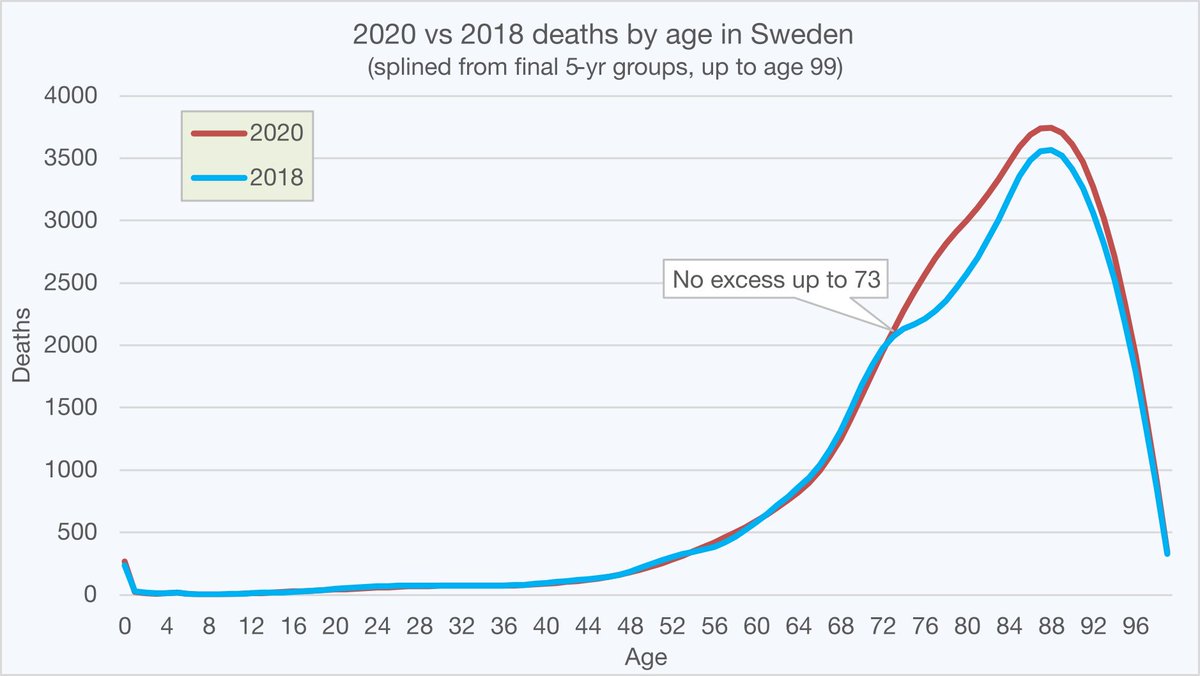
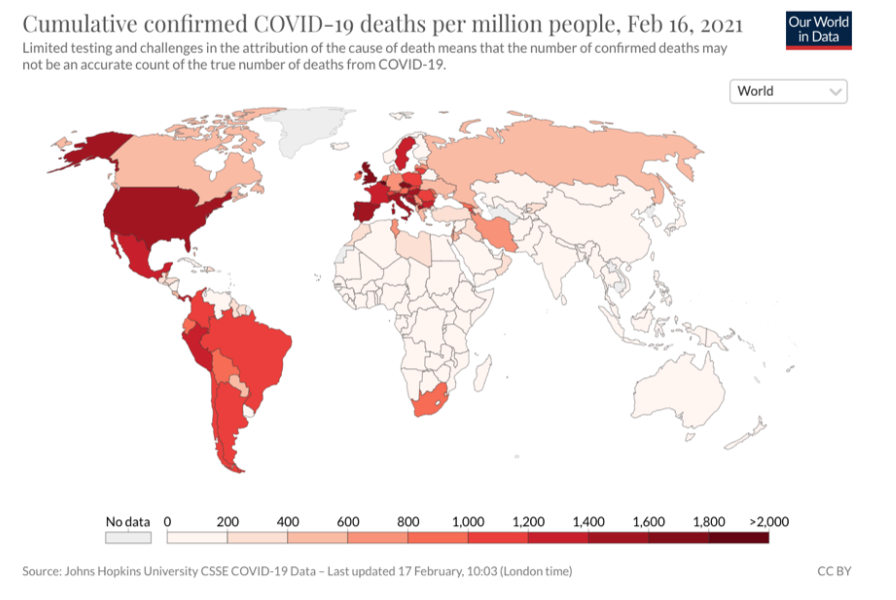
The pandemic is real. Excess deaths were observed in many countries. Not all countries were affected in the same way due to pre-existing immunity, the health status of the population and demographics (the proportion of elderly in the population) 2/n
https://t.co/65elPq3gp5
COVID 19 presents a high risk for the very few and negligible risk for the many.
The infection fatality rate in different age groups:
<19 y, IFR= 0.003%
20-49 y: IFR= 0.02%
50-69 y: 0.5%
>70y, IFR=
Not everybody is susceptible to the virus. If reinfected, pre-existing immunity from related viruses gives protection from developing the disease or from developing serious symptoms.
4/n
“The evidence that a subset of people has a cross-reactive T cell repertoire through exposure to related coronaviruses is
FACTS NOT FEAR
Covid 19 is a disease caused by the SARS-CoV-2 virus. SARS-CoV-2 is one of 7 coronaviruses known to man. 1/n
The pandemic is real. Excess deaths were observed in many countries. Not all countries were affected in the same way due to pre-existing immunity, the health status of the population and demographics (the proportion of elderly in the population) 2/n
https://t.co/65elPq3gp5
COVID 19 presents a high risk for the very few and negligible risk for the many.
The infection fatality rate in different age groups:
<19 y, IFR= 0.003%
20-49 y: IFR= 0.02%
50-69 y: 0.5%
>70y, IFR=
Not everybody is susceptible to the virus. If reinfected, pre-existing immunity from related viruses gives protection from developing the disease or from developing serious symptoms.
4/n
“The evidence that a subset of people has a cross-reactive T cell repertoire through exposure to related coronaviruses is
You May Also Like









Department List of UCAS-China PROFESSORs for ANSO, CSC and UCAS (fully or partial) Scholarship Acceptance
1) UCAS School of physical sciences Professor
https://t.co/9X8OheIvRw
2) UCAS School of mathematical sciences Professor
3) UCAS School of nuclear sciences and technology
https://t.co/nQH8JnewcJ
4) UCAS School of astronomy and space sciences
https://t.co/7Ikc6CuKHZ
5) UCAS School of engineering
6) Geotechnical Engineering Teaching and Research Office
https://t.co/jBCJW7UKlQ
7) Multi-scale Mechanics Teaching and Research Section
https://t.co/eqfQnX1LEQ
😎 Microgravity Science Teaching and Research
9) High temperature gas dynamics teaching and research section
https://t.co/tVIdKgTPl3
10) Department of Biomechanics and Medical Engineering
https://t.co/ubW4xhZY2R
11) Ocean Engineering Teaching and Research
12) Department of Dynamics and Advanced Manufacturing
https://t.co/42BKXEugGv
13) Refrigeration and Cryogenic Engineering Teaching and Research Office
https://t.co/pZdUXFTvw3
14) Power Machinery and Engineering Teaching and Research
1) UCAS School of physical sciences Professor
https://t.co/9X8OheIvRw
2) UCAS School of mathematical sciences Professor
3) UCAS School of nuclear sciences and technology
https://t.co/nQH8JnewcJ
4) UCAS School of astronomy and space sciences
https://t.co/7Ikc6CuKHZ
5) UCAS School of engineering
6) Geotechnical Engineering Teaching and Research Office
https://t.co/jBCJW7UKlQ
7) Multi-scale Mechanics Teaching and Research Section
https://t.co/eqfQnX1LEQ
😎 Microgravity Science Teaching and Research
9) High temperature gas dynamics teaching and research section
https://t.co/tVIdKgTPl3
10) Department of Biomechanics and Medical Engineering
https://t.co/ubW4xhZY2R
11) Ocean Engineering Teaching and Research
12) Department of Dynamics and Advanced Manufacturing
https://t.co/42BKXEugGv
13) Refrigeration and Cryogenic Engineering Teaching and Research Office
https://t.co/pZdUXFTvw3
14) Power Machinery and Engineering Teaching and Research