
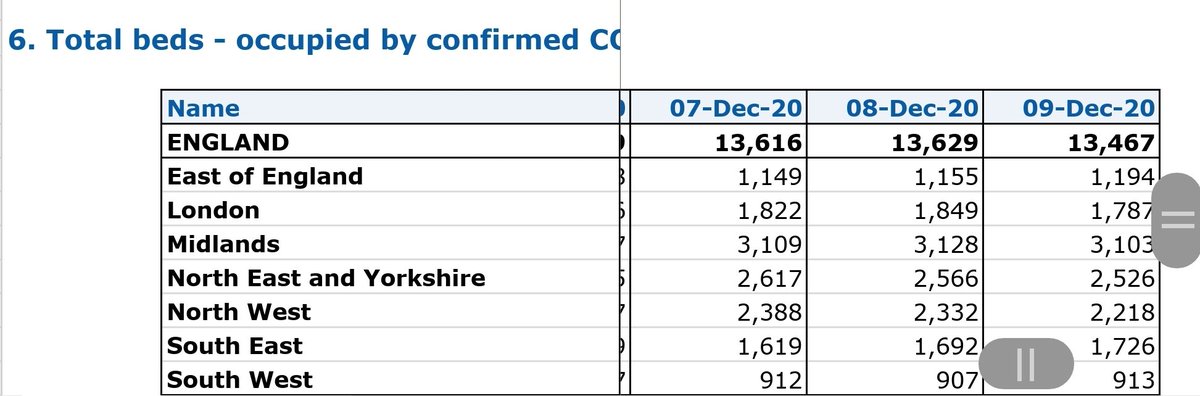
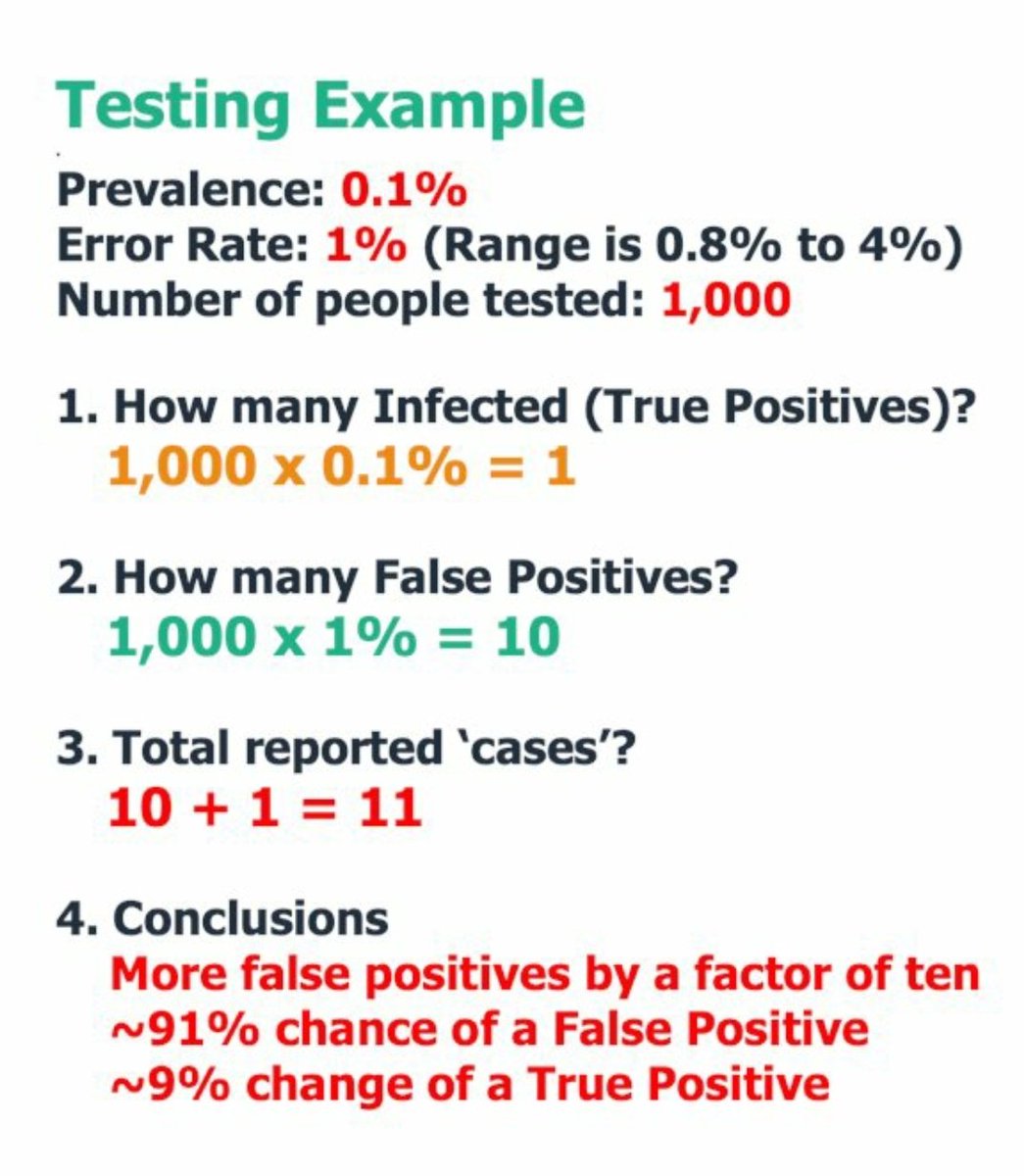
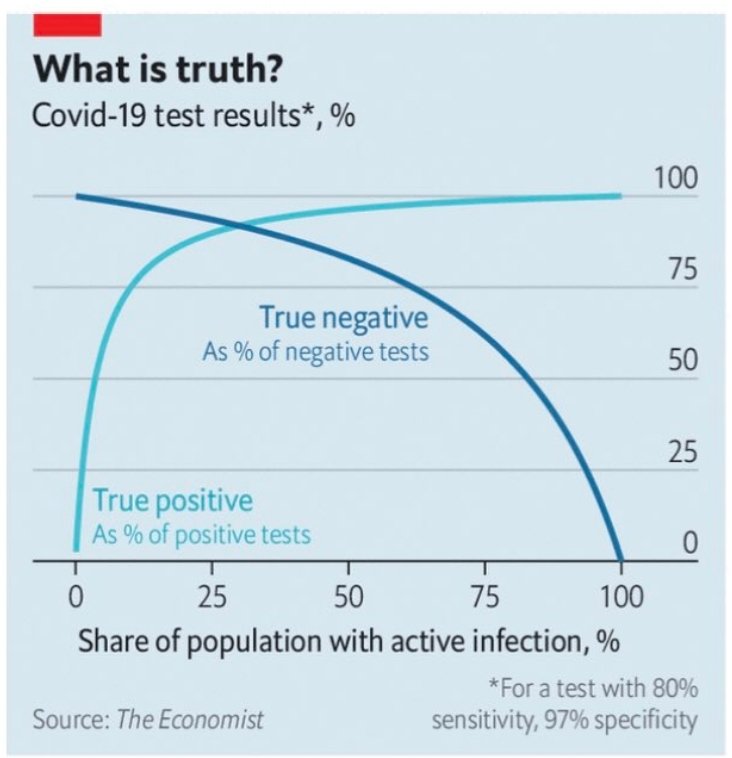
BAYES' THEOREM: The basic reason we get so many false positives to COVID19. The disease is so rare that the number of false positives greatly outnumbers the people who truly have the disease: THE MATHS:
https://t.co/oLHyxYJW9H

https://t.co/29FNwq0Qw2
"The national statistician has downgraded its estimate of coronavirus in England on October 17 to just 4.89 people per 10,000." or ~ 0.05%. That means that only 1 in 2000 people may be carrying SARS related viral RNA fragments which could be 2 months old. https://t.co/XqpNaY6BzQ
— Robin Monotti FRSA MA BSc (@robinmonotti) December 8, 2020
https://t.co/rthjPRJWeB
ITALY: CONFIRMED BY ITALIAN HEALTH SERVICE: False positives to Covid19 test as diagnosis are 95%. Legal cases started against testing under charges of fraud to procure public funding, false alarm, ideological false, and manslaughter. pic.twitter.com/C9b7BbzdKa
— Robin Monotti FRSA MA BSc (@robinmonotti) November 25, 2020
#BAYESTHEOREM MEDICAL MASS TESTING CALCULATOR:
— Robin Monotti FRSA MA BSc (@robinmonotti) December 9, 2020
Try it yourself to understand how many false positives you get by changing minor variables: \U0001f447https://t.co/7wVMvrpgAW pic.twitter.com/PHbweWK1TK
https://t.co/kFnQVoCspb
LATERAL FLOW: False positive rate of "0.4% with a sensitivity of 58% and specificity of 99.6%, would mean that 100\u2009000 people being tested would find 630 positives\u2014of which only 230 would actually have covid-19, while 400 would be false positives.
— Robin Monotti FRSA MA BSc (@robinmonotti) November 17, 2020
https://t.co/8hsZ1hNjD7
Official estimates from mass testing in England (including asymptomatic) puts Covid19 "infections" at 0.9% https://t.co/2ljzi9YfKN
— Robin Monotti FRSA MA BSc (@robinmonotti) December 11, 2020
@lucyfrazermp 20/11:
— Edmund Fordham (@EdmundFordham) November 28, 2020
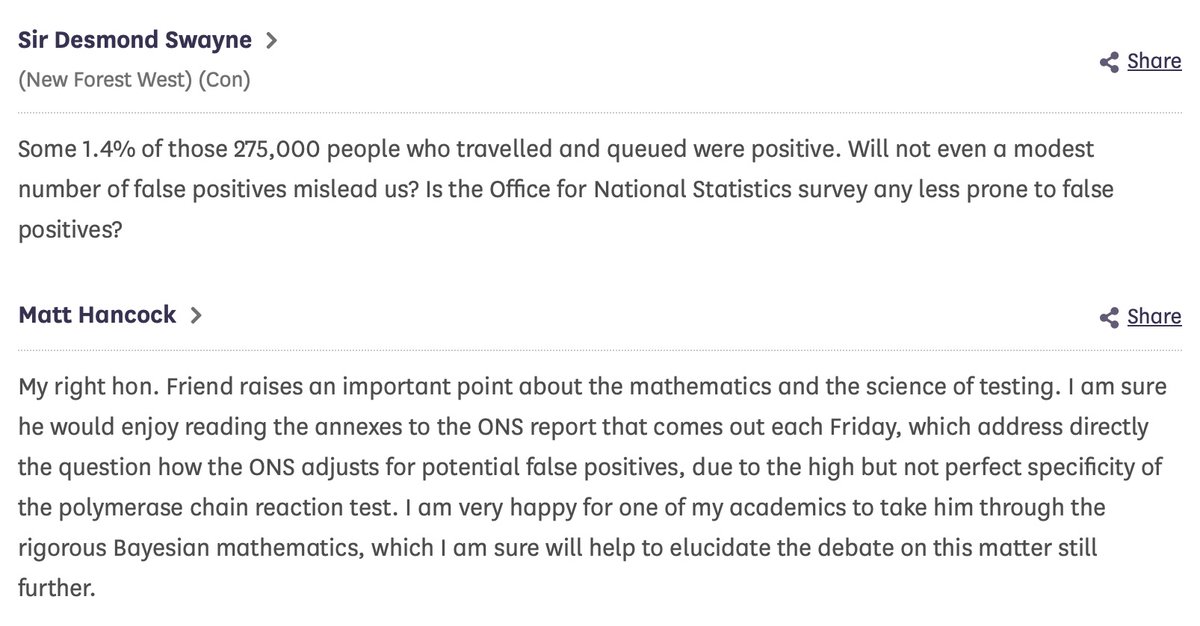
2. Apparently @MattHancock tells HoC 17/09 how ONS \u201cadjusts for False Positives\u201d. Looked it up.@DesmondSwayne asks;@MattHancock doesn\u2019t answer.
Obfuscates with \u201crigorous Bayesian mathematics\u201d
\u201cOne of his academics" will \u201ctake him through it\u201d
(thread) pic.twitter.com/42YO9vaioy
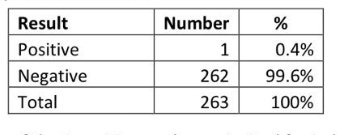
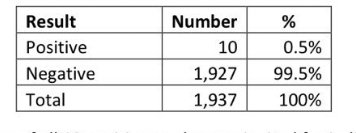
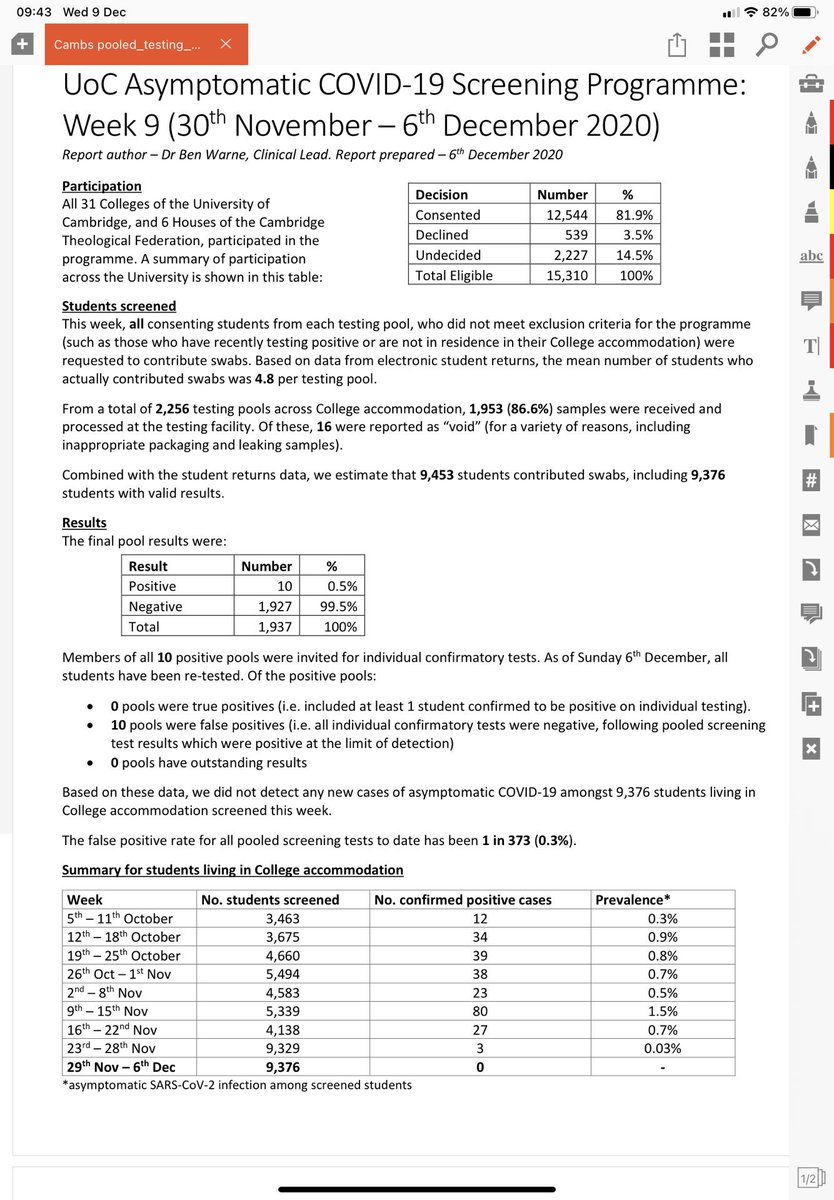
#BAYESTHEOREM @ Cambridge University. 0.4% of 262 students came back as positive after the first "test". All came back as negative after the second. Government only tests once. ONS would say there is 0.4% prevalence instead it's 0%. pic.twitter.com/zeAQAAOeRN
— Robin Monotti FRSA MA BSc (@robinmonotti) December 13, 2020
https://t.co/pZcFlMBKEZ
"I am very happy for one of my academics to take him through the rigorous Bayesian mathematics, which I am sure will help to elucidate the debate on this matter still further." @MattHancock to @DesmondSwaynehttps://t.co/pZcFlMBKEZ
— Robin Monotti FRSA MA BSc (@robinmonotti) December 15, 2020
https://t.co/aidVGWOVqH
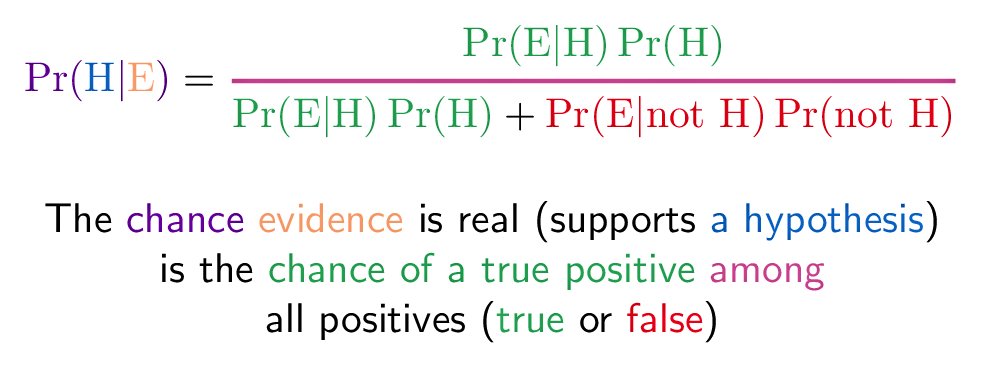
Numerical details aside, the use of Bayes's theorem and the principle described are valid. Taught in epidemiology courses.
— \u05e4\u05e8\u05d5\u05e4' \u05d0\u05d9\u05d9\u05dc \u05e9\u05d7\u05e8 (@prof_shahar) December 16, 2020
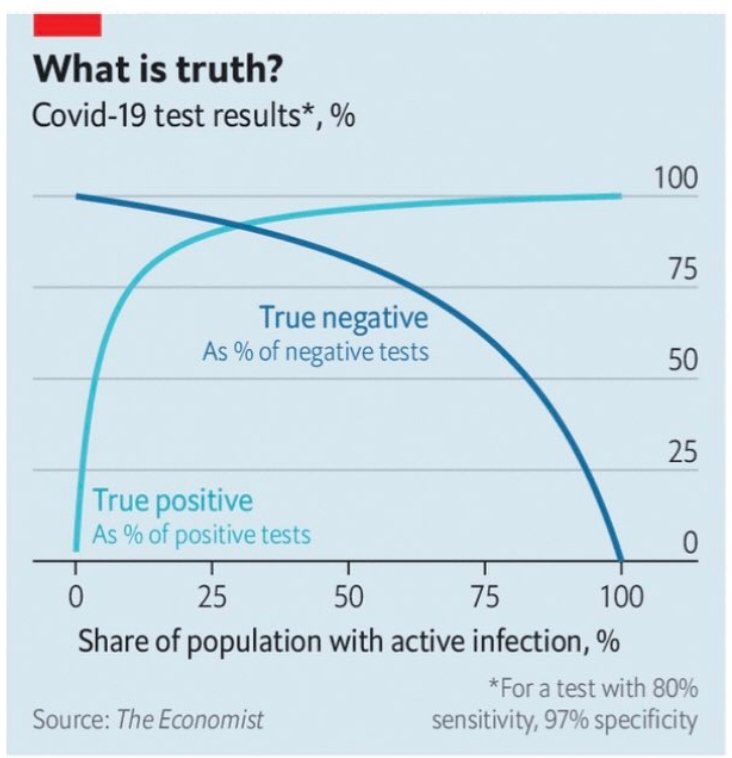
Extreme example. If disease prevalence is zero, predictive value of positive test is zero. Every positive is false positive.
A similar graph in the thread pic.twitter.com/ddvBe36OmU
\u26a0\ufe0fWHO WARNING ON BAYES THEOREM & TESTING \u26a0\ufe0f
— Robin Monotti FRSA MA BSc (@robinmonotti) December 16, 2020
"Healthcare providers are encouraged to take into consideration testing results along with clinical signs and symptoms, confirmed status of any contacts"https://t.co/GkRJzdn70b pic.twitter.com/jXPQDqqnVE
More from Robin Monotti FRSA MA BSc
The evidence based science shows that medical face masks for the healthy do not alter rates of community transmission of SARSCoV2 while they contribute to the plastic pollution of planet. Cloth & masks of other materials increase rates of infection through nebulization spread.
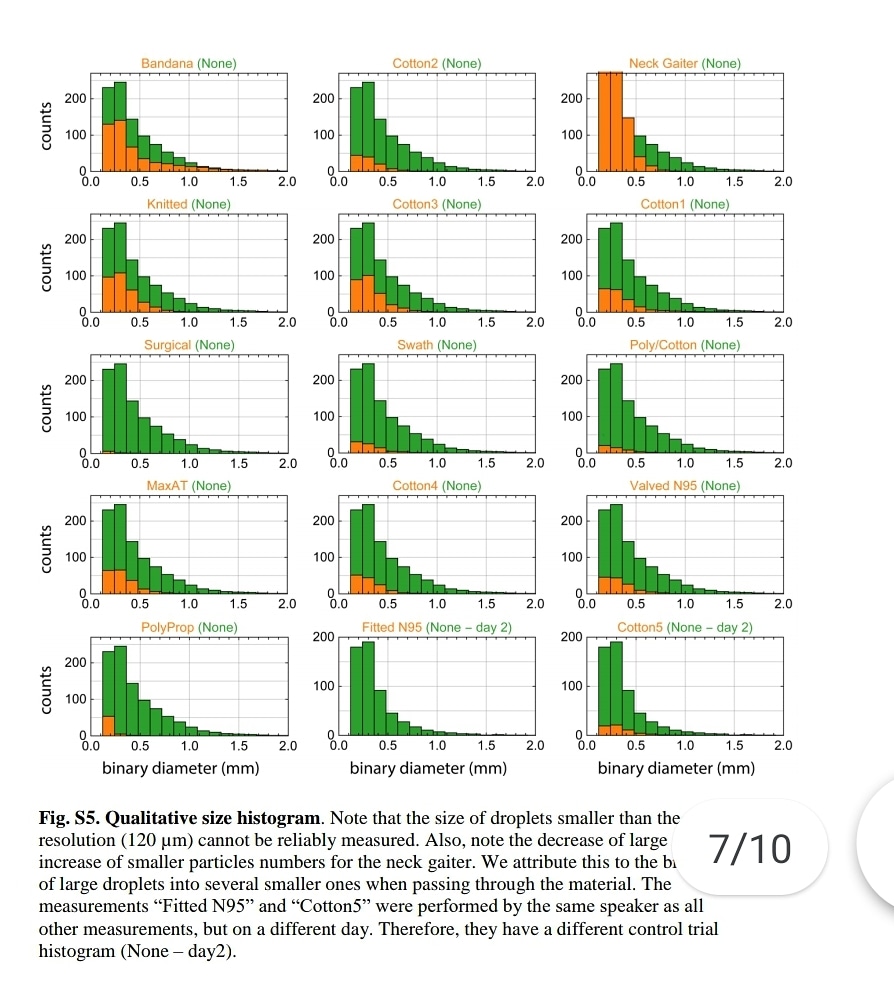
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."
https://t.co/jBQlWRxcEL
Influenza like illness rates 3 times higher with cloth masks when compared to control group:
https://t.co/djT0mfutv9
Prof. Carl Heneghan, Oxford University: "The high quality trial evidence for cloth masks suggest they increase your rate of reinfection."

Please note, droplets smaller than 120 microns can't be measured. SARSCoV2 is 0.14 microns. This means that the nebulization effect of medical masks could not be measured, not that it does not happen. ⬇️
The really small aerosols <1 μm [the ones that pass through ALL surgical masks] can penetrate all the way to the alveoli - the basic units for gas exchange
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."
https://t.co/jBQlWRxcEL
Influenza like illness rates 3 times higher with cloth masks when compared to control group:
https://t.co/djT0mfutv9
Prof. Carl Heneghan, Oxford University: "The high quality trial evidence for cloth masks suggest they increase your rate of reinfection."
Please note, droplets smaller than 120 microns can't be measured. SARSCoV2 is 0.14 microns. This means that the nebulization effect of medical masks could not be measured, not that it does not happen. ⬇️
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."https://t.co/jBQlWRxcEL pic.twitter.com/XeKYFmjsGs
— Robin Monotti (@robinmonotti) January 15, 2021
The really small aerosols <1 μm [the ones that pass through ALL surgical masks] can penetrate all the way to the alveoli - the basic units for gas exchange
4/In humans, larger aerosols deposit in upper throat, nose, & tracheobronchial region of the lung. Medium-sized aerosols mostly deposit in small airways further down. The really small aerosols <1 \u03bcm can penetrate all the way to the alveoli - the basic units for gas exchange. 4/7 pic.twitter.com/9ZJb4JrZqI
— Dr. Ali Nouri (@AliNouriPhD) December 29, 2020
Twitter removed 800 followers from my account today. People have been writing saying twitter automatically unfollowed me for them. Follow me on Parler @robinmonotti & Telegram https://t.co/o5rFaSrCpa to bypass this.
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
I have already left both Facebook & Instagram. We need to keep agile.
They will try to ban Parler, blaming it for Capitol theatre. I think Telegram may survive as it's not based in the
Yes Telegram owner @durov received & accepted what effectively is an award, not a partnership: the Young Global Leaders membership of the World Economic Forum in 2017. Does this mean he passes users info on? I don't think so.
This is what @Snowden had to say about @durov. Since then Telegram introduced the option of end to end encrypted chats not saved in Telegram servers. These private chats cannot be forwarded, and none of the participants can capture screenshots of
Trust us not to turn over data. Trust us not to read your messages. Trust us not to close your channel. Maybe @Durov is an angel. I hope so! But angels have fallen before. Telegram should have been working to make channels decentralized\u2014meaning outside their control\u2014for years.
— Edward Snowden (@Snowden) December 30, 2017
I have now re-examined this document:
It clearly does indicate both the risks of bacterial infection & to prescribe broad spectrum antibiotics as part of treatment:
"Collect blood cultures for bacteria that cause pneumonia and sepsis, ideally before antimicrobial therapy. DO NOT
delay antimicrobial therapy"
"6. Management of severe COVID-19: treatment of co-infections
Give empiric antimicrobials [broad spectrum antibiotics] to treat all likely pathogens causing SARI and sepsis as soon as possible, within 1 hour
of initial assessment for patients with sepsis."
"Empiric antibiotic treatment should be based on the clinical diagnosis (community-acquired
pneumonia, health care-associated pneumonia [if infection was acquired in health care setting] or sepsis), local epidemiology &
susceptibility data, and national treatment guidelines"
"When there is ongoing local circulation of seasonal influenza, empiric therapy with a neuraminidase inhibitor [anti-viral influenza drugs] should
be considered for the treatment for patients with influenza or at risk for severe disease."
On the 19th March 2020 the WHO released this guidance intended for healthcare workers (HCWs), healthcare managers and IPC teams at the facility level & at national and district/provincial level:https://t.co/C4aV2BnMPj pic.twitter.com/tCk1EyLskV
— Robin Monotti (@robinmonotti) December 21, 2020
It clearly does indicate both the risks of bacterial infection & to prescribe broad spectrum antibiotics as part of treatment:
"Collect blood cultures for bacteria that cause pneumonia and sepsis, ideally before antimicrobial therapy. DO NOT
delay antimicrobial therapy"
"6. Management of severe COVID-19: treatment of co-infections
Give empiric antimicrobials [broad spectrum antibiotics] to treat all likely pathogens causing SARI and sepsis as soon as possible, within 1 hour
of initial assessment for patients with sepsis."
"Empiric antibiotic treatment should be based on the clinical diagnosis (community-acquired
pneumonia, health care-associated pneumonia [if infection was acquired in health care setting] or sepsis), local epidemiology &
susceptibility data, and national treatment guidelines"
"When there is ongoing local circulation of seasonal influenza, empiric therapy with a neuraminidase inhibitor [anti-viral influenza drugs] should
be considered for the treatment for patients with influenza or at risk for severe disease."
Italian researchers: vaccines will not work against SARSCoV2 because this virus does not only replicate in human cells like other viruses, this one replicates through bacteria too. This is the fundamental reason why antibiotics work & vaccines will not:
Here is the Italian-EU scientific study indicating SARSCoV2 replicates in bacteria, not only human cells, and that is why antibiotics work and these vaccines will not:
"The preliminary results suggest that SARS-CoV-2 replicates in bacterial
2 of the 4 authors of the study work at the European Commission. Another works at an Italian medical research facility called Craniomed: https://t.co/EETSM3nb3T
You can find all of CRANIOMED's Carlo Brogna's published scientific research articles here, take a look:
Here is the Italian-EU scientific study indicating SARSCoV2 replicates in bacteria, not only human cells, and that is why antibiotics work and these vaccines will not:
"The preliminary results suggest that SARS-CoV-2 replicates in bacterial
2 of the 4 authors of the study work at the European Commission. Another works at an Italian medical research facility called Craniomed: https://t.co/EETSM3nb3T
You can find all of CRANIOMED's Carlo Brogna's published scientific research articles here, take a look:
More from Category c19

1/ Thread – THE YEAR OF THE RAT
“15 days to slow the spread” began one year ago. It was March 2020, the Year of the Rat. Never was any year more fitting of the name. Never in history have the people been betrayed so callously, flagrantly and absolutely by their alleged leaders.

2/ They were betrayed by their WHO
3/ and their national health
4/ They were betrayed by medical
5/ and their peer
“15 days to slow the spread” began one year ago. It was March 2020, the Year of the Rat. Never was any year more fitting of the name. Never in history have the people been betrayed so callously, flagrantly and absolutely by their alleged leaders.
2/ They were betrayed by their WHO
3/ and their national health
4/ They were betrayed by medical
Despite ignorance by many in the West, this article by The Lancet is a powerful endorsement of China\u2019s successful pandemic response. Hate to read stories by those paparazzi journalists who are experts at spinning but have little knowledge of science. https://t.co/Q8rKwwTPsI pic.twitter.com/436BEmx9nl
— Chen Weihua \uff08\u9648\u536b\u534e\uff09 (@chenweihua) October 16, 2020
5/ and their peer
6/ Eurosurveillance, a journal whose editors coincidentally includes Mr. Drosten, takes only a single day for the peer review process and publishes the hastily compiled PCR protocol on January 22. https://t.co/cWX3UdKeID
— Pace \U0001f642 (@theotherphilipp) February 25, 2021

1/: Avicenna was a Persian scientist, who lived 1000 years ago. He put two lambs in separate cages, which had the same health conditions. But only one lamb could see a wolf that was put in a third cage. The observations were astounding. (h/t @farmer_student) ⬇️a thread⬇️
2/: Both lambs were provided with the same feed. Also, the weight was exactly the same when the experiment started. Several months later, the lamb with sight on the wolf became cranky, restless, weak, and showed a significant weight loss and signs of poor development.
3/: The lamb that was under chronic stress as it was placed in a situation of constant apparent danger died eventually. 🐑🪦 In fact, the wolf did not pose a danger at all, but this was beyond the lamb's perception.
4/: This experiment showed that increased levels of the stress hormone cortisol have a bad impact on the metabolism of mammals. And 1000 years after this experiment, we are facing a similar situation again but with the difference that we are aware of the impact of stress.
5/: Currently, we are overwhelmed with medial and governmental propaganda with respect to a common cold virus (that might hypothetically be more lethal though) that doesn't do harm to the majority of the people. Extreme global measures are taken.
2/: Both lambs were provided with the same feed. Also, the weight was exactly the same when the experiment started. Several months later, the lamb with sight on the wolf became cranky, restless, weak, and showed a significant weight loss and signs of poor development.
3/: The lamb that was under chronic stress as it was placed in a situation of constant apparent danger died eventually. 🐑🪦 In fact, the wolf did not pose a danger at all, but this was beyond the lamb's perception.
4/: This experiment showed that increased levels of the stress hormone cortisol have a bad impact on the metabolism of mammals. And 1000 years after this experiment, we are facing a similar situation again but with the difference that we are aware of the impact of stress.
5/: Currently, we are overwhelmed with medial and governmental propaganda with respect to a common cold virus (that might hypothetically be more lethal though) that doesn't do harm to the majority of the people. Extreme global measures are taken.
Cortisol is known as the 'stress hormone' and is a silent killer. Cortisol levels are increased by:
— Dr. Simon \u30c4 (@goddeketal) February 17, 2021
\U0001f449\U0001f3fc Fear & anxiety
\U0001f449\U0001f3fc Constant stress
\U0001f449\U0001f3fc Social isolation
The media propagated fear and political measures are counterproductive. They shorten our lives. https://t.co/6BZ34pVBjw

1) THERE IS A VERY REAL, CREDIBLE AND SIGNIFICANT DANGER THAT mRNA SPIKE PROTEIN THERAPIES WILL INDUCE PRION OR PRION-LIKE DISEASE
A paper from 2016 shows that prion and prion-like proteins can also spread and propagate from cell to cell through macropinocytosis. It is also
2) noted that the Spike Protein of SARS-CoV-2 can enter cells through macropinocytosis, without the presence of the entire virion. Given the recent Tweet to me by @endocdoc, where he recently saw a patient develop Creutzfeld-Jakob after COVID-19, the extant paper showing CJD
3) CJD after COVID-19 infection and the recent death of the head of Astra-Zeneca research from CJD should be concerning to all. Especially if he gave himself the AZ therapy during Stage 1 or Stage 2 trials. This would give a possible timeframe for onset.
Again, all Spike Protein
4) mRNA and DNA should be paused until long term animal studies can be
5)
https://t.co/PWOgyPoG5d
A paper from 2016 shows that prion and prion-like proteins can also spread and propagate from cell to cell through macropinocytosis. It is also
2) noted that the Spike Protein of SARS-CoV-2 can enter cells through macropinocytosis, without the presence of the entire virion. Given the recent Tweet to me by @endocdoc, where he recently saw a patient develop Creutzfeld-Jakob after COVID-19, the extant paper showing CJD
3) CJD after COVID-19 infection and the recent death of the head of Astra-Zeneca research from CJD should be concerning to all. Especially if he gave himself the AZ therapy during Stage 1 or Stage 2 trials. This would give a possible timeframe for onset.
Again, all Spike Protein
4) mRNA and DNA should be paused until long term animal studies can be
5)
https://t.co/PWOgyPoG5d
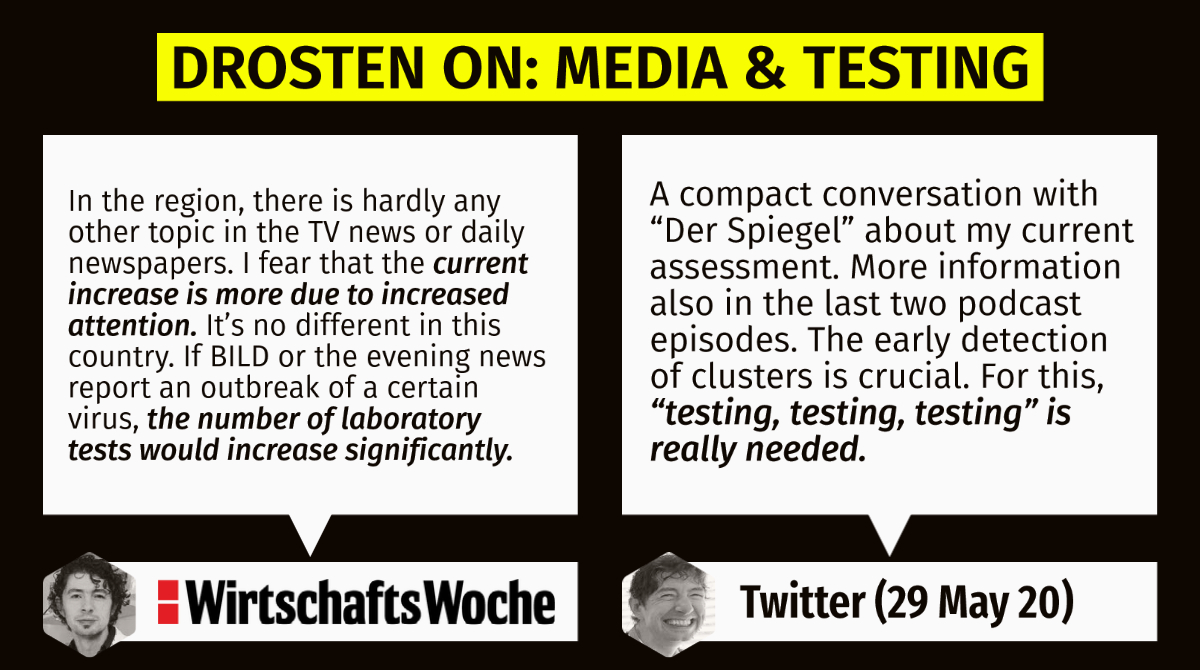
1/: The inventor of the corona PCR-Test @c_drosten is one of the #protagonists of the current crisis. He is known for involving himself in contradictions. In 2014, he gave a legendary #interview to @wiwo (https://t.co/jzTRh5Suhc) that I will address in this ⬇️short thread⬇️.
2/: The interview is significant because @c_drosten made totally sane statements back then that follow the principle of common sense. Considering his involvement in the "genesis of the current pandemic", his assertions appear in an entirely different
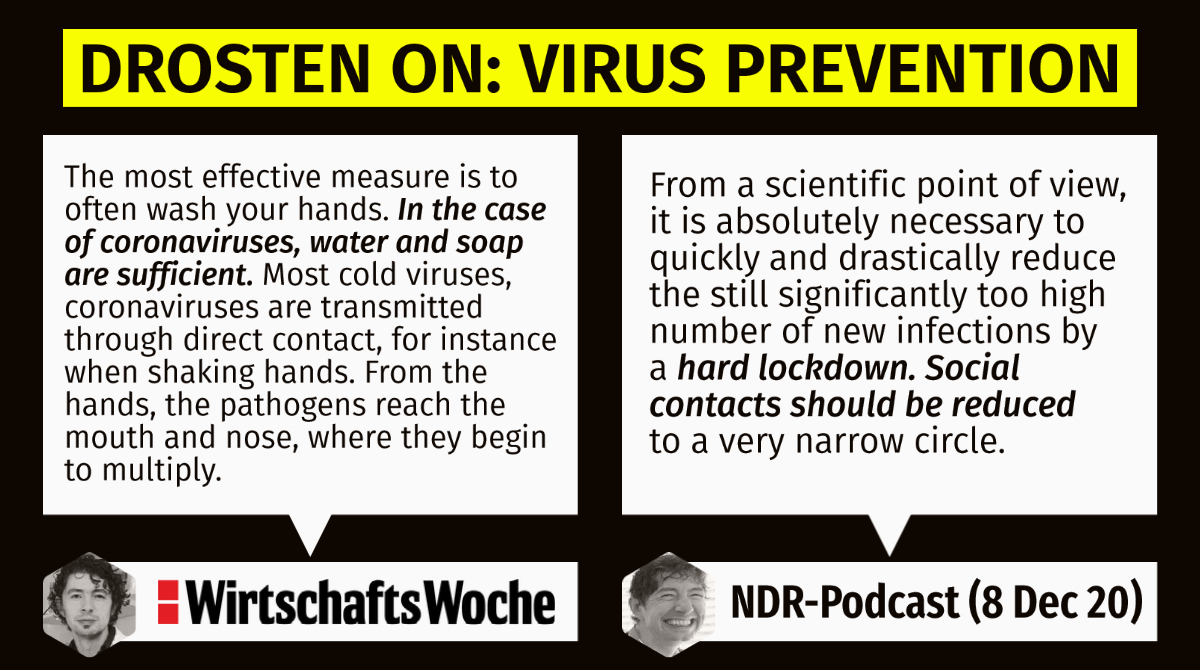
3/: In 2014, for instance, washing the hands was sufficient against being infected by coronaviruses. Several years he demands measures that destroy national economies and social life worldwide.
4/: Young @c_drosten also severely criticized the fact that Saudi Arabia used the PCR method to detect potential infections. From his point of view, that specific method could lead to many irrelevant cases. Nowadays, his view shifted his opinion towards 'collective punishment'.
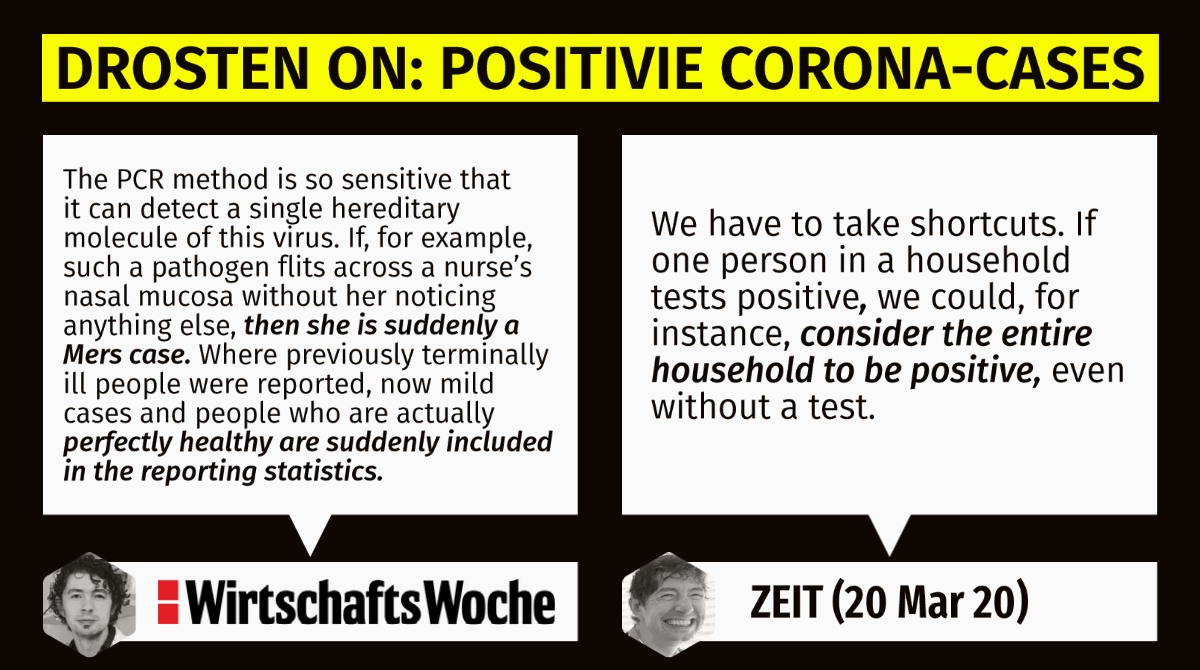
5/: Whereas he demands "testing, testing, testing" nowadays and spreads panic and fear via (social) media, he heavily condemned that behaviour of Saudi media in 2014. On top of that, he expressed his concern that medial panic could increase the number of lab tests significantly.
2/: The interview is significant because @c_drosten made totally sane statements back then that follow the principle of common sense. Considering his involvement in the "genesis of the current pandemic", his assertions appear in an entirely different
The genesis of a pandemic.
— Pace \U0001f642 (@theotherphilipp) February 25, 2021
The #Corona crisis began with a panopticon of absurd events, improbable coincidences and outright lies.
Time for a review of the impossibilities.
A thread \U0001f9f5 pic.twitter.com/PLbETVv2p8
3/: In 2014, for instance, washing the hands was sufficient against being infected by coronaviruses. Several years he demands measures that destroy national economies and social life worldwide.
4/: Young @c_drosten also severely criticized the fact that Saudi Arabia used the PCR method to detect potential infections. From his point of view, that specific method could lead to many irrelevant cases. Nowadays, his view shifted his opinion towards 'collective punishment'.
5/: Whereas he demands "testing, testing, testing" nowadays and spreads panic and fear via (social) media, he heavily condemned that behaviour of Saudi media in 2014. On top of that, he expressed his concern that medial panic could increase the number of lab tests significantly.











