CodyyyGardner Categories Health

But TRASH "health" agencies & experts continue w/their Wear A Mask campaign & suppress niacin
Bacterial Pneumonia and Other Health Risks of Wearing Masks Alarm Doctors https://t.co/8eKmIaxeMQ
— Toni (@Landau_18901) January 3, 2021
https://t.co/1DRUO9L3ap
And remember, @CDCgov already concluded in systematic review of 14 RCTs that masks don't mitigate influenza spread, and a meta analysis further evidenced that even N95 masks make no difference vs cloth masks, meaning that no masks - not even N95 - workhttps://t.co/mSwdz7U6tM
— 3PIDEMIOLOGY (@3PIDEMIOLOGY) December 31, 2020







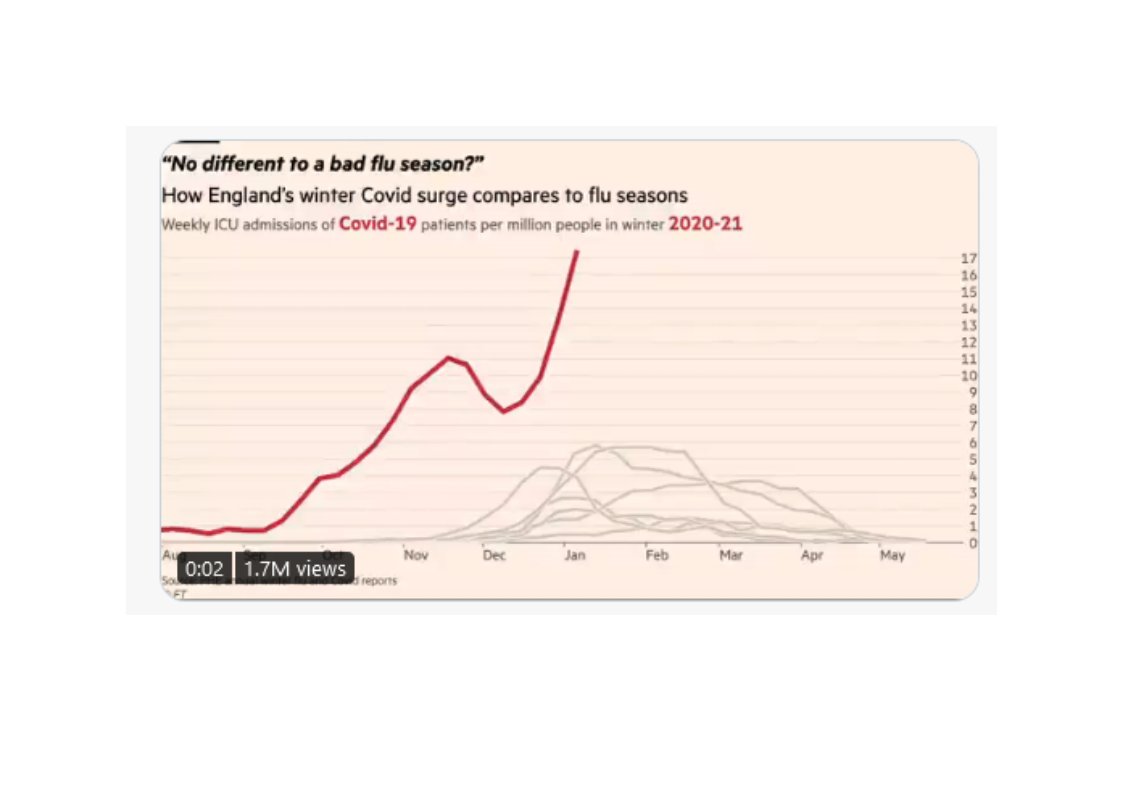
NEW: a common response to reports of hospitals struggling this winter is "it\u2019s no different to a bad flu season!"
— John Burn-Murdoch (@jburnmurdoch) January 7, 2021
I\u2019ve tracked down historical data on flu ICU admissions, including winter 2017-18, a record high.
Here\u2019s how England\u2019s Covid winter compares to a bad flu season \U0001f4f9 pic.twitter.com/tsExrDZM31
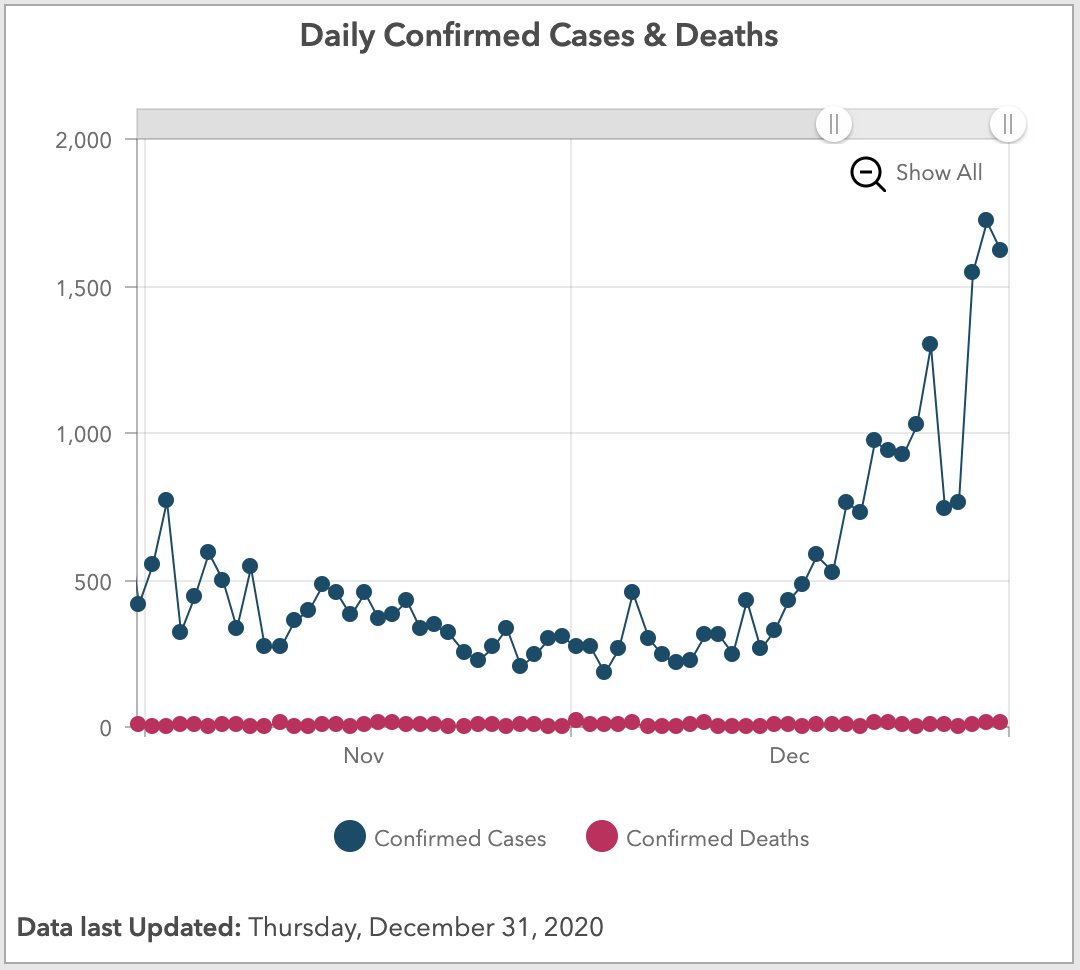
27/42 Some sceptics arguing covid-19 tests are inaccurate. PCR tests not 100% accurate but hospital inpatient testing accuracy much increased by frequency of testing (typically admission, days 3 & 6/7, then weekly). This means very low numbers of overall false positives.
28/42 Some sceptics argue that the published covid-19 positive inpatient numbers include both those admitted with covid-19 and those who acquired covid-19 in hospital. And that there are significant numbers of patients who have acquired covid-19 in hospital.
29/42 Covid-19 positive test data has always included anyone testing positive, irrespective of initial diagnosis. And the NHS has always acknowledged that hospital acquired (nosocomial) infection is a big issue. Hospitals are working incredibly hard to control it….
30/42 …The NHS regularly and completely transparently publishes nosocomial infection data, by hospital. But neither issue affects the degree of pressure that hospitals are under. Every inpatient, irrespective of initial diagnosis/infection source, occupies a hospital bed.














So, in terms of people in Melbourne freaking out about Sydney's seemingly lacking response to the current outbreak, coupled with the new cases in Victoria - this is going to trigger a trauma response.
The lockdown was traumatising.
How much, depends on the individual.
When you have a trauma response, it is physically terrifying. Your adrenaline might surge. You could feel afraid. You could feel angry. You might react by lashing out. You might shut down. You might have anxiety that it is all "going to happen again".
Or that you don't think you could survive another lockdown, because you barely survived the last one.
These are all natural and normal responses, and I know they are hard, and I am so sorry if you're feeling this fear.
I don't know what is going to happen.
I do hope that you can do your best to be safe. Try to take each moment as it comes, do the best you can do to get by.
Please find helplines below.
Beyond Blue Covid Mental Health call 1800 512 348 (also online
Australians, this time of year is extremely difficult for many people. A thread (in progress) for contacts;
— MJ Leaver (@MJ_Leaver) December 18, 2017
000 if life is in danger.
1300 659 467 : National Suicide Call Back Service (15+)
1800 55 1800 : Kid's Helpline (5-25yrs)
1800 184 527 : QLife (LGBTQI folks)

348,601 "ever-#snus users had about 60% lower Parkinson's disease risk compared with never-snus users."
https://t.co/YHB9FKkUtQ
30,000 British doctors followed for 60 years: "current smokers at baseline had a 30% lower risk of
#MedicalNicotine
Nicotine is beneficial for people with #ADHD. Research on adults and adolescents with ADHD shows that nicotine patches improve focus and attention, and reduce hyperactivity &
ADHD: "Nicotine ...may have properties similar to stimulant medications (e.g., Ritalin) used to treat ADHD. [It] may increase attention and reduce hyperactivity & impulsivity."https://t.co/l9QVnJHBhl#MedicalNicotine #ADHD #ADHDAwareness #Autism #Neurodiversity #Neurodivergent
— ClovisSangrail (@ClovisSangrail4) January 3, 2021
#MedicalNicotine
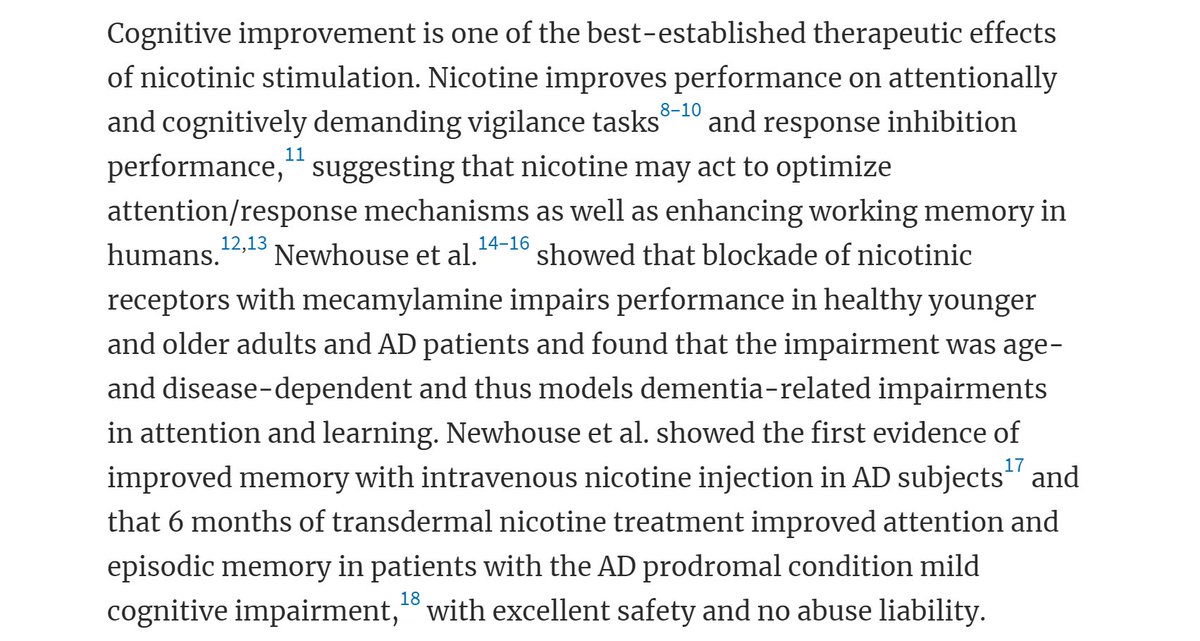
Nicotine reduces symptoms of Alzheimer's disease (AD).
https://t.co/Tht2Y8CZiN
#MedicalNicotine
Nicotine is beneficial for people with schizophrenia. More than 70% of people with schizophrenia smoke.
#SaferNicotine alternatives could help them as therapy, and to not die from
#MedicalNicotine
Nicotine, "(either 2 mg nicotine gum or 7 mg transdermal nicotine patch) potentiates [enhances] the therapeutic properties of neuroleptics in treating Tourette's syndrome... A single patch may be effective for a variable number of






