
As someone who has studied healthcare handoffs for a while, I can’t stop thinking about the Presidential one coming up. I see I’m not the only one. But this is not like any handoff. My nerdy 🧵 #MedTwitter #Inauguration2021
More from Health










🚨Important changes to lockdown/self-isolation regulations from 5pm
The Health Protection (Coronavirus, Restrictions) (All Tiers and Self-Isolation) (England) (Amendment) Regulations 2021
£800 'house party' FPN & police can now access track & trace data
https://t.co/k9XCpVsXhC
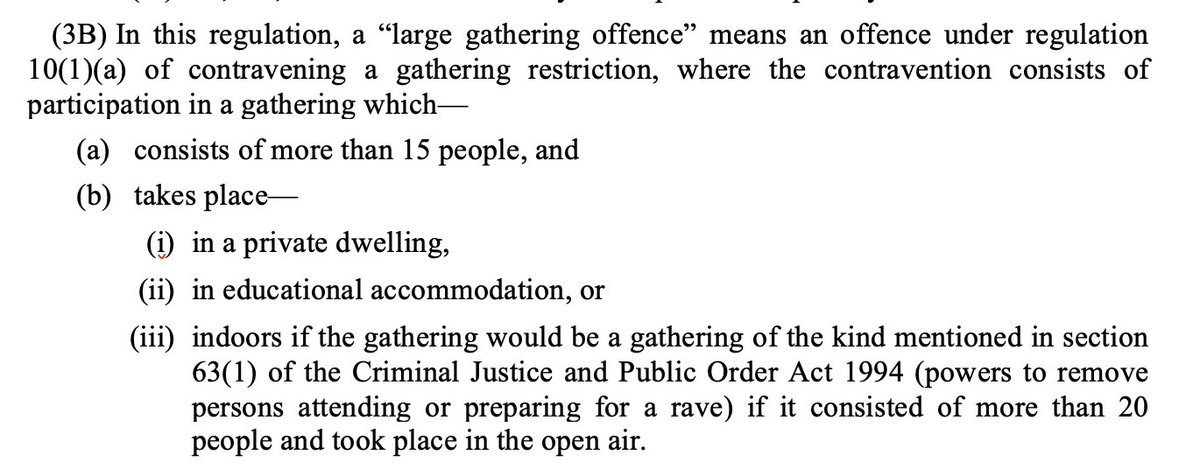
“Large gathering offence”
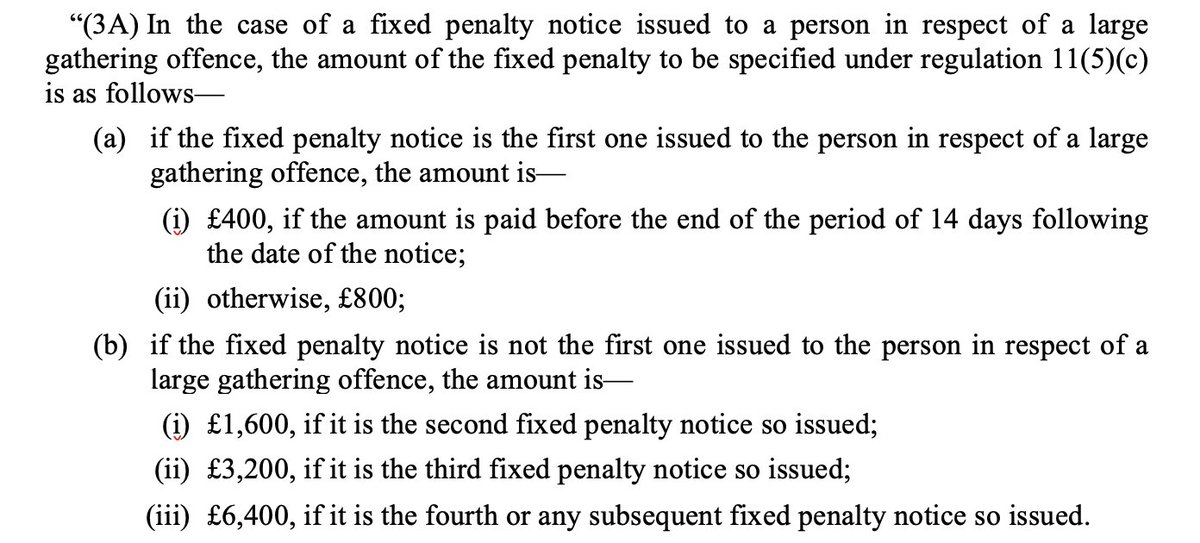
As trailed by Home Secretary last week there is now a fixed penalty notice of £800 (or £400 if you pay within 14 days) for participating in an gathering of over 15 people in a private residence
Fixed Penalty Notices double for each subsequent “large gathering offence” up to £6,400
Compare:
- Ordinary fixed penalty notice is £200 or £100 if paid in 14 days
- Holding or being involved in the holding of a gathering of over 30 people is £10,000
Second big change:
Since September has been a legal requirement to sell-isolate if you test positive/notified by Track & Trace of exposure to someone else who tested positive
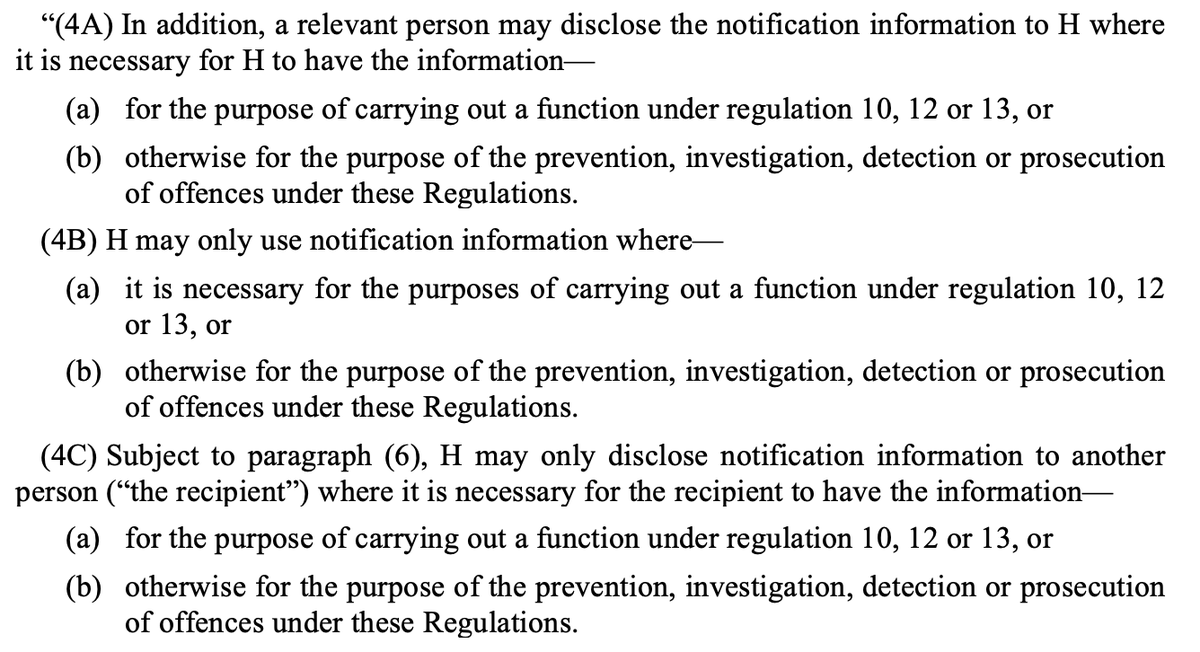
Police can now be given access to NHS Track & Trace data if for the purpose of enforcement/prosecution
This will make it easier for police to enforce people breaking self-isolation rules. Currently there has been practically no enforcement.
Data says only a small proportion of people meant to be self-isolating are fully doing so.
The Health Protection (Coronavirus, Restrictions) (All Tiers and Self-Isolation) (England) (Amendment) Regulations 2021
£800 'house party' FPN & police can now access track & trace data
https://t.co/k9XCpVsXhC
“Large gathering offence”
As trailed by Home Secretary last week there is now a fixed penalty notice of £800 (or £400 if you pay within 14 days) for participating in an gathering of over 15 people in a private residence
Fixed Penalty Notices double for each subsequent “large gathering offence” up to £6,400
Compare:
- Ordinary fixed penalty notice is £200 or £100 if paid in 14 days
- Holding or being involved in the holding of a gathering of over 30 people is £10,000
Second big change:
Since September has been a legal requirement to sell-isolate if you test positive/notified by Track & Trace of exposure to someone else who tested positive
Police can now be given access to NHS Track & Trace data if for the purpose of enforcement/prosecution
This will make it easier for police to enforce people breaking self-isolation rules. Currently there has been practically no enforcement.
Data says only a small proportion of people meant to be self-isolating are fully doing so.
Very important that obvious failures with Track and Trace and self-isolation (study late last year said 18% of people complying https://t.co/dhJUZ7Pm0l) are not painted as an enforcement issue. Plainly not. Would just pass buck to police who have almost no capacity to enforce https://t.co/Eb4Kl5Ze0E
— Adam Wagner (@AdamWagner1) January 25, 2021

You May Also Like






Facebook originally a CIA program called "LifeLog".
LifeLog, via DARPA, terminated on Feb 4th, 2004.
Facebook was launched on Feb 4th, 2004.
Many of the LifeLog team became execs at FB.
Zuckerberg is a figurehead.
CIA allowed Cambridge to help Trump win
https://t.co/enzOXDCogV

Pentagon Kills LifeLog
LifeLog, via DARPA, terminated on Feb 4th, 2004.
Facebook was launched on Feb 4th, 2004.
Many of the LifeLog team became execs at FB.
Zuckerberg is a figurehead.
CIA allowed Cambridge to help Trump win
https://t.co/enzOXDCogV
Project: Lifelog
— Robert Horan (@Robby12692) December 13, 2018
Started by DARPA in 1999, the goal of Lifelog was to create a database on civilians without their knowledge, and track everything they do.
The project "ended" on Feb 4th, 2004.
Facebook began the exact same day.
The CIA funneled tens of millions into Facebook. pic.twitter.com/r7hwF0v9kh
Pentagon Kills LifeLog
