
As someone who has studied healthcare handoffs for a while, I can’t stop thinking about the Presidential one coming up. I see I’m not the only one. But this is not like any handoff. My nerdy 🧵 #MedTwitter #Inauguration2021
More from Health


this simple, counter narrative fact keeps cropping up all over the world.
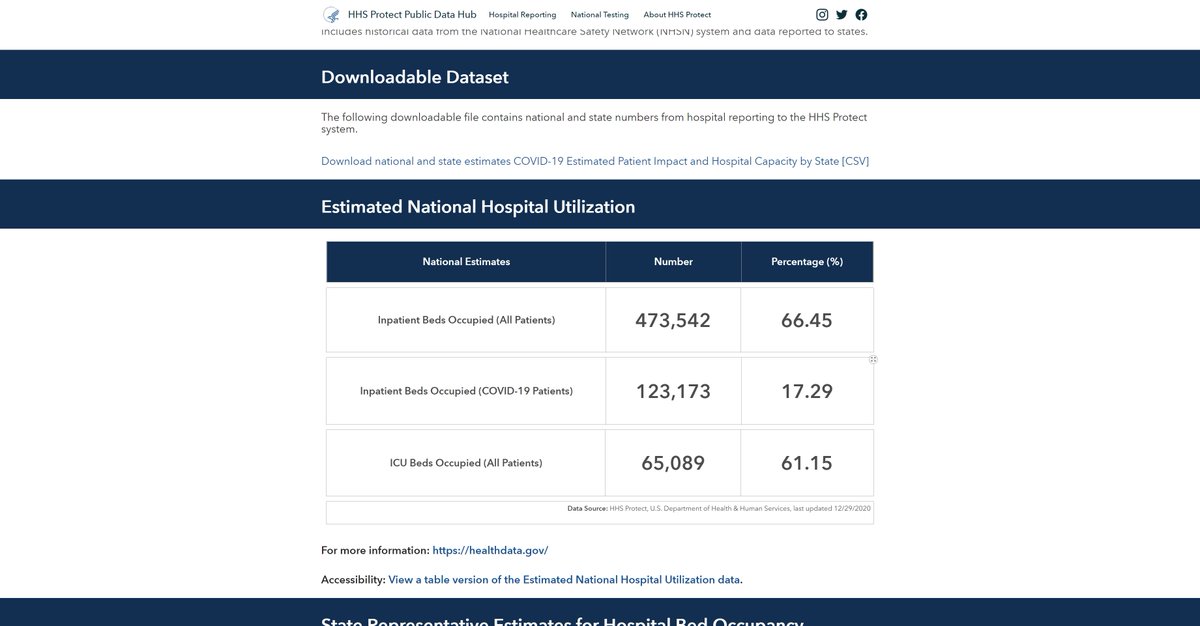
hospital and ICU utilization has been and remains low this year.
it's terribly curious that so few of these monitoring tools provide historical baselines.
getting them is like pulling teeth.
we might think of this as an oversight until you see stuff like this:
this woman was arrested for filming and sharing the fact that their are empty hospitals in the UK.
that's full blown soviet. what possible honest purpose does that
this is the action of a police state and a propaganda ministry, not a well intentioned government and a public heath agency.
"we cannot let people see the truth for fear they might base their actions on real facts" is not much of a mantra for just governance.

90% full ICU sounds scary until you realize that 90-100% full is normal in flu season.
staffed ICU beds are expensive to leave empty. it's like flying with 15% of the plane empty. hospitals don't do that.
and all US hospitals are mandated to be able to flex to 120% ICU.
the US is currently at historically low ICU utilization for this time of year.
61% is "you're all going to go out of business" territory as is 66% full hospital use.
can you blame them for mining CARES act money? they'll die without it.
hospital and ICU utilization has been and remains low this year.
it's terribly curious that so few of these monitoring tools provide historical baselines.
getting them is like pulling teeth.
It took a Freedom of Information request but @Covid19DataUK acquired 2017-2019 averages for England hospitalizations.
— Yinon Weiss (@yinonw) December 31, 2020
2020 had 18% fewer hospitalizations than prior years.
All around the world, using hospital data without context of prior years is just a fear generating lie. pic.twitter.com/DJDpqhIQuw
we might think of this as an oversight until you see stuff like this:
this woman was arrested for filming and sharing the fact that their are empty hospitals in the UK.
that's full blown soviet. what possible honest purpose does that
this is the action of a police state and a propaganda ministry, not a well intentioned government and a public heath agency.
"we cannot let people see the truth for fear they might base their actions on real facts" is not much of a mantra for just governance.
90% full ICU sounds scary until you realize that 90-100% full is normal in flu season.
staffed ICU beds are expensive to leave empty. it's like flying with 15% of the plane empty. hospitals don't do that.
and all US hospitals are mandated to be able to flex to 120% ICU.
the US is currently at historically low ICU utilization for this time of year.
61% is "you're all going to go out of business" territory as is 66% full hospital use.
can you blame them for mining CARES act money? they'll die without it.



You May Also Like



Keep dwelling on this:
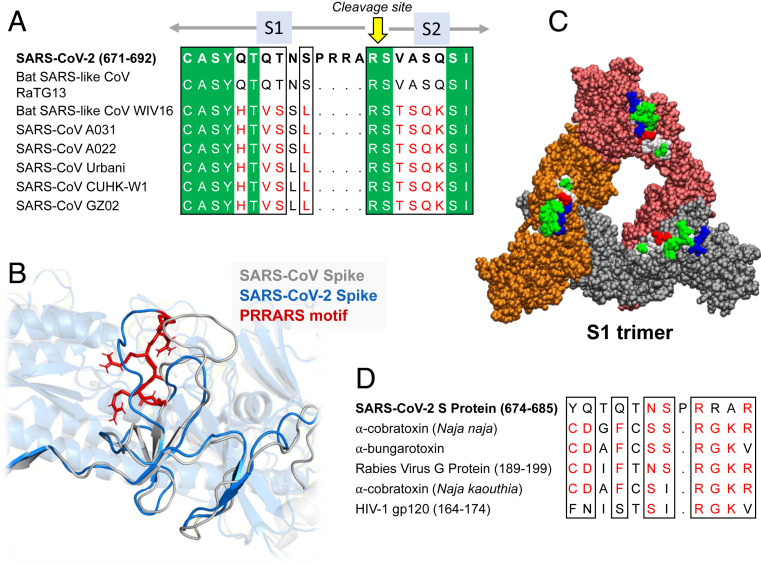
Further Examination of the Motif near PRRA Reveals Close Structural Similarity to the SEB Superantigen as well as Sequence Similarities to Neurotoxins and a Viral SAg.
The insertion PRRA together with 7 sequentially preceding residues & succeeding R685 (conserved in β-CoVs) form a motif, Y674QTQTNSPRRAR685, homologous to those of neurotoxins from Ophiophagus (cobra) and Bungarus genera, as well as neurotoxin-like regions from three RABV strains
(20) (Fig. 2D). We further noticed that the same segment bears close similarity to the HIV-1 glycoprotein gp120 SAg motif F164 to V174.
https://t.co/EwwJOSa8RK
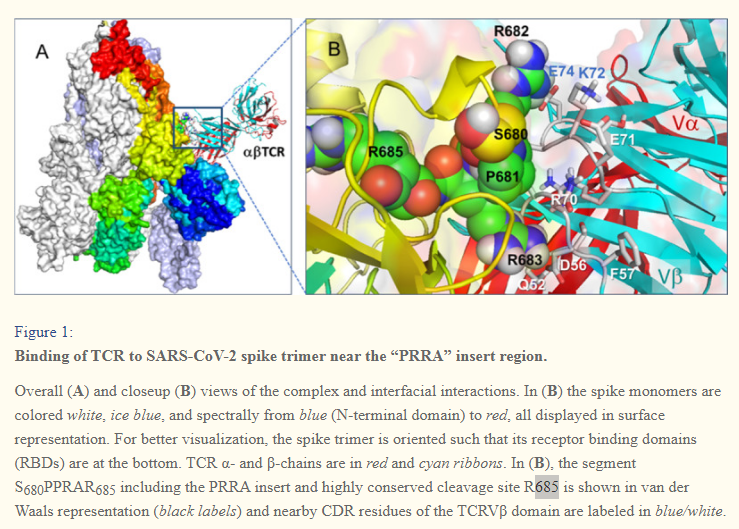
In (B), the segment S680PPRAR685 including the PRRA insert and highly conserved cleavage site *R685* is shown in van der Waals representation (black labels) and nearby CDR residues of the TCRVβ domain are labeled in blue/white
https://t.co/BsY8BAIzDa
Sequence Identity %
https://t.co/BsY8BAIzDa
Y674 - QTQTNSPRRA - R685
Similar to neurotoxins from Ophiophagus (cobra) & Bungarus genera & neurotoxin-like regions from three RABV strains
T678 - NSPRRA- R685
Superantigenic core, consistently aligned against bacterial or viral SAgs
Further Examination of the Motif near PRRA Reveals Close Structural Similarity to the SEB Superantigen as well as Sequence Similarities to Neurotoxins and a Viral SAg.
The insertion PRRA together with 7 sequentially preceding residues & succeeding R685 (conserved in β-CoVs) form a motif, Y674QTQTNSPRRAR685, homologous to those of neurotoxins from Ophiophagus (cobra) and Bungarus genera, as well as neurotoxin-like regions from three RABV strains
(20) (Fig. 2D). We further noticed that the same segment bears close similarity to the HIV-1 glycoprotein gp120 SAg motif F164 to V174.
https://t.co/EwwJOSa8RK
In (B), the segment S680PPRAR685 including the PRRA insert and highly conserved cleavage site *R685* is shown in van der Waals representation (black labels) and nearby CDR residues of the TCRVβ domain are labeled in blue/white
https://t.co/BsY8BAIzDa
Sequence Identity %
https://t.co/BsY8BAIzDa
Y674 - QTQTNSPRRA - R685
Similar to neurotoxins from Ophiophagus (cobra) & Bungarus genera & neurotoxin-like regions from three RABV strains
T678 - NSPRRA- R685
Superantigenic core, consistently aligned against bacterial or viral SAgs












