
What is the basis of this?
I've been seeing a lot of discussion around the dosage gaps recommended by government for the Astra/Oxford & Pfizer/BioNTech vaccines. My thoughts on the potential benefits & risks of such an approach, and the need for much greater transparency around these decisions. Thread.
What is the basis of this?
1) the first dose is likely to confer some degree of protection against disease, so better to roll this out as fast as possible, and
2) that for Oxford/Astra efficacy may be higher when the gap between doses is greater.
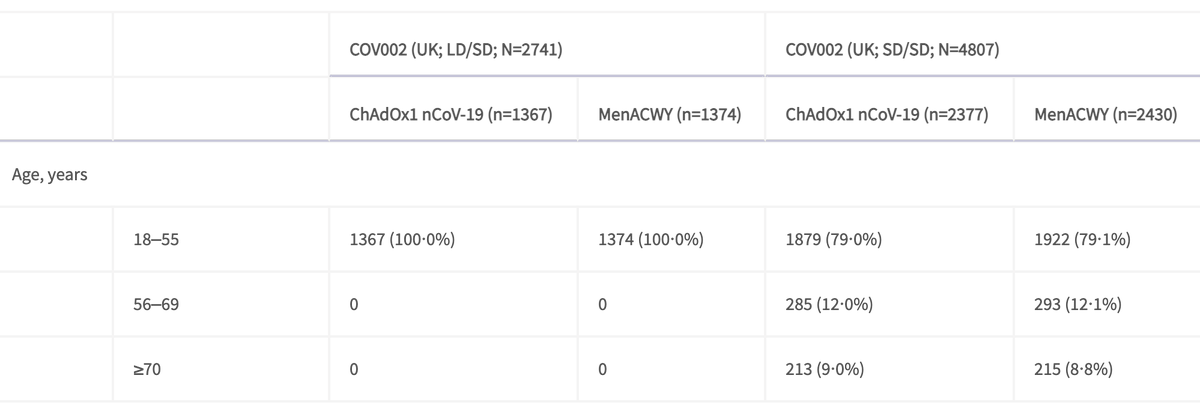
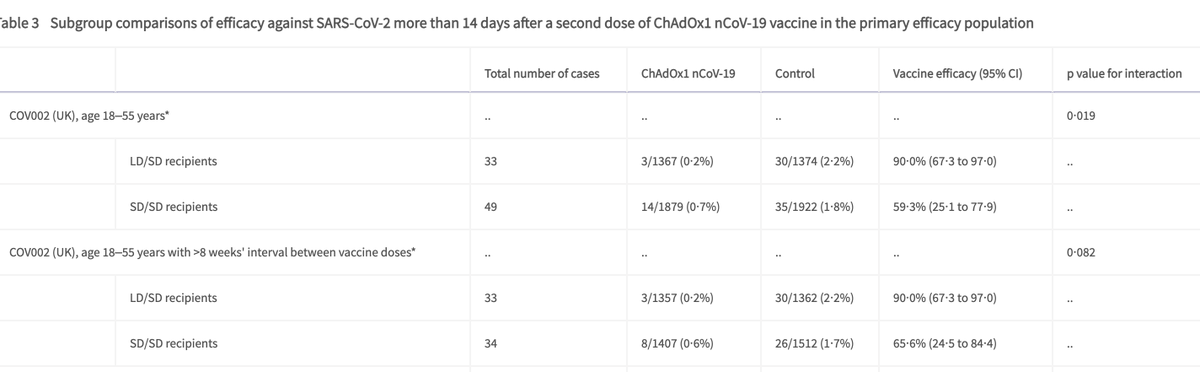
Vaccine efficacy among 18-55 yr olds SD/SD dosing was 59% vs LD/SD dosing at 90%.
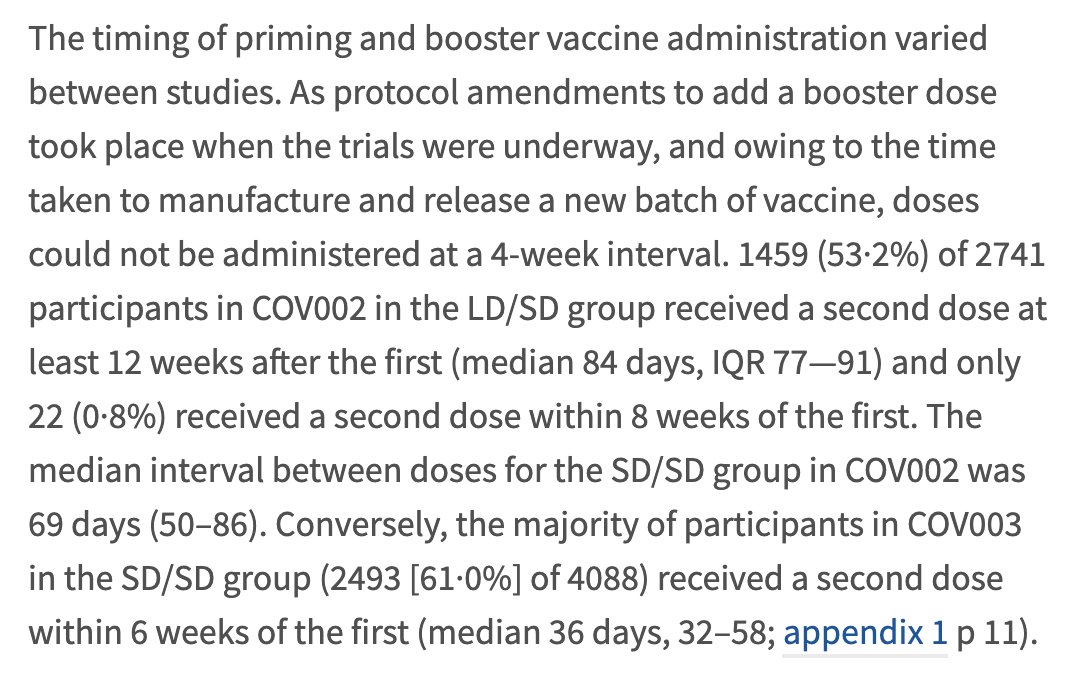
Is this due to dosing, or differences in gaps between doses?
Differences in gaps don't appear to impact efficacy in this analysis.
https://t.co/9yaSAyHcKR
It looks like the first dose prevented all severe disease (although numbers were small) in the SARS-CoV-2 vaccine group compared to vaccine control after the first 21 days of vaccination, and <14 days after the 2nd dose.
https://t.co/966V4EYw13
U.S. is now considering idea of a single vaccination shot, delaying shot #2 until months later. Last wk, I thought that was a bad idea \u2013 the trials that found 95% efficacy were 2 shots; why add extra complexity & a new curveball. But facts on the ground demand a rethink. (1/7)
— Bob Wachter (@Bob_Wachter) December 31, 2020
1. Resources for roll-out are limited & fixed & we need to optimise how best to use them within limitations
2. There isn't significant decline in immunity after the 3 wk mark
3. Later dosing will not affect overall efficacy
A key part of the rationale appears to be a bottleneck in vaccine supply (rather than roll-out).
https://t.co/mccavkBGeb
The reasoning is public now https://t.co/ZkO1k0yqlL.
— Volker Schulz (@portefeuillefun) December 31, 2020
More from Deepti Gurdasani
Thread on the recent report on the possible risk of increased death associated with the new UK variant (B117)- with a discussion of the evidence around this, and what this means.
First, there is strong evidence to support increased transmissibility of B117 - current estimates of increased transmissibility range between 30-70% - from epidemiological evidence examining the differential rate of growth of B117 with respect to other variants & increase in R
There is also evidence from PHE contact studies that the risk of transmission from those carrying the B117 variant is ~50% greater than with other non-B117 variants.
Increased transmissibility, even if a variant has the same fatality rate can increase deaths substantially, because the rate of growth of cases is higher- & more cases means more deaths.
Increased fatality rates also increase deaths- but do so
So how was risk of death with the variant studied?
We don't routinely sequence all samples for the virus. We've found that the variant has a particular deletion which means that some PCR tests on samples with the variant give a different read-out when the variant is present.
First, there is strong evidence to support increased transmissibility of B117 - current estimates of increased transmissibility range between 30-70% - from epidemiological evidence examining the differential rate of growth of B117 with respect to other variants & increase in R
There is also evidence from PHE contact studies that the risk of transmission from those carrying the B117 variant is ~50% greater than with other non-B117 variants.
Increased transmissibility, even if a variant has the same fatality rate can increase deaths substantially, because the rate of growth of cases is higher- & more cases means more deaths.
Increased fatality rates also increase deaths- but do so
How dangerous are the B.1.1.7 and 501Y.V2 hyper-transmissible strains?
— Eric Topol (@EricTopol) January 11, 2021
by @AdamJKucharski @CFR_orghttps://t.co/aycWMN3b5h
h/t @Karl_Lauterbach pic.twitter.com/JlaFzzP06t
So how was risk of death with the variant studied?
We don't routinely sequence all samples for the virus. We've found that the variant has a particular deletion which means that some PCR tests on samples with the variant give a different read-out when the variant is present.
This is the exact problem with our government's thinking & response- despite this strategy of 'tolerating deaths' and half-way measures having spectacularly failed, it's quite amazing that our govt still hasn't learned anything, & continues to promote a policy of death. Thread
Had we adopted an elimination strategy early on, rather than one of tolerating a certain level of infection, we wouldn't be here now. The reason we're here is because the govt never committed to elimination.
We eased lockdown in May when infection levels were much higher than when other countries in Europe did this. The govt was warned about this, but did this to 'help the economy'. Not only did this lead us into the 2nd wave, the need for further lockdowns harmed the economy further
It's very clear from global evidence that we cannot 'tolerate a level of community transmission' and maintain 'R at or just below 1', which has been our governments policy for a long time. This isn't sustainable & very rapidly gets out of control, leading to exponential rises
Coupled with late action to contain these surges, not only does this lead to many more deaths, and much more morbidity with Long COVID, it also creates a fertile ground for viral mutations to accumulate with a greater risk of adaptation, which is exactly what happened in the UK
U.K. needs to confront
— Esther McVey (@EstherMcVey1) January 2, 2021
\u2018The challenge that faces us is to decide - are we going to try to pursue the elimination of Covid-19 regardless of the costs or decide on a tolerable level of deaths (like we do with the flu) in order to return to a normal life?\u2019
https://t.co/9hWbHIPJUq
Had we adopted an elimination strategy early on, rather than one of tolerating a certain level of infection, we wouldn't be here now. The reason we're here is because the govt never committed to elimination.
We eased lockdown in May when infection levels were much higher than when other countries in Europe did this. The govt was warned about this, but did this to 'help the economy'. Not only did this lead us into the 2nd wave, the need for further lockdowns harmed the economy further
It's very clear from global evidence that we cannot 'tolerate a level of community transmission' and maintain 'R at or just below 1', which has been our governments policy for a long time. This isn't sustainable & very rapidly gets out of control, leading to exponential rises
Coupled with late action to contain these surges, not only does this lead to many more deaths, and much more morbidity with Long COVID, it also creates a fertile ground for viral mutations to accumulate with a greater risk of adaptation, which is exactly what happened in the UK
We've been falsely told 'schools are safe', 'don't drive community transmission', & teachers don't have a higher risk of infection repeatedly by govt & their advisors- to justify some of the most negligent policies in history. 🧵
data shows *both* primary & secondary school teachers are at double the risk of confirmed infection relative to comparable positivity in the general population. ONS household infection data also clearly show that children are important sources of transmission.
Yet, in the parliamentary select meeting today, witnesses like Jenny Harries repeated the same claims- that have been debunked by the ONS data, and the data released by the @educationgovuk today. How many lives have been lost to these lies? How many more people have long COVID?
has repeatedly pointed out errors & gaps in the ONS reporting of evidence around risk of infection among teachers- and it's taken *months* to get clarity on this. The released data are a result of months of campaigning by her, the @NEU and others.
Rather than being transparent about the risk of transmission in school settings & mitigating this, the govt (& many of its advisors) has engaged in dismissing & denying evidence that's been clear for a while. Evidence from the govt's own surveys. And global evidence.
Why?
Questions have to be asked about the evidence Jenny Harries gave to the Education Committee today about the risk to teachers.
— Adam Hamdy (@adamhamdy) January 19, 2021
Was she aware of this data?
If not, why wasn\u2019t she properly briefed?#COVID19 #schools https://t.co/4wa1PyAJld pic.twitter.com/eqFjaA1zYC
data shows *both* primary & secondary school teachers are at double the risk of confirmed infection relative to comparable positivity in the general population. ONS household infection data also clearly show that children are important sources of transmission.
Yet, in the parliamentary select meeting today, witnesses like Jenny Harries repeated the same claims- that have been debunked by the ONS data, and the data released by the @educationgovuk today. How many lives have been lost to these lies? How many more people have long COVID?
has repeatedly pointed out errors & gaps in the ONS reporting of evidence around risk of infection among teachers- and it's taken *months* to get clarity on this. The released data are a result of months of campaigning by her, the @NEU and others.
Rather than being transparent about the risk of transmission in school settings & mitigating this, the govt (& many of its advisors) has engaged in dismissing & denying evidence that's been clear for a while. Evidence from the govt's own surveys. And global evidence.
Why?
Brief thread to debunk the repeated claims we hear about transmission not happening 'within school walls', infection in school children being 'a reflection of infection from the community', and 'primary school children less likely to get infected and contribute to transmission'.
I've heard a lot of scientists claim these three - including most recently the chief advisor to the CDC, where the claim that most transmission doesn't happen within the walls of schools. There is strong evidence to rebut this claim. Let's look at
Let's look at the trends of infection in different age groups in England first- as reported by the ONS. Being a random survey of infection in the community, this doesn't suffer from the biases of symptom-based testing, particularly important in children who are often asymptomatic
A few things to note:
1. The infection rates among primary & secondary school children closely follow school openings, closures & levels of attendance. E.g. We see a dip in infections following Oct half-term, followed by a rise after school reopening.
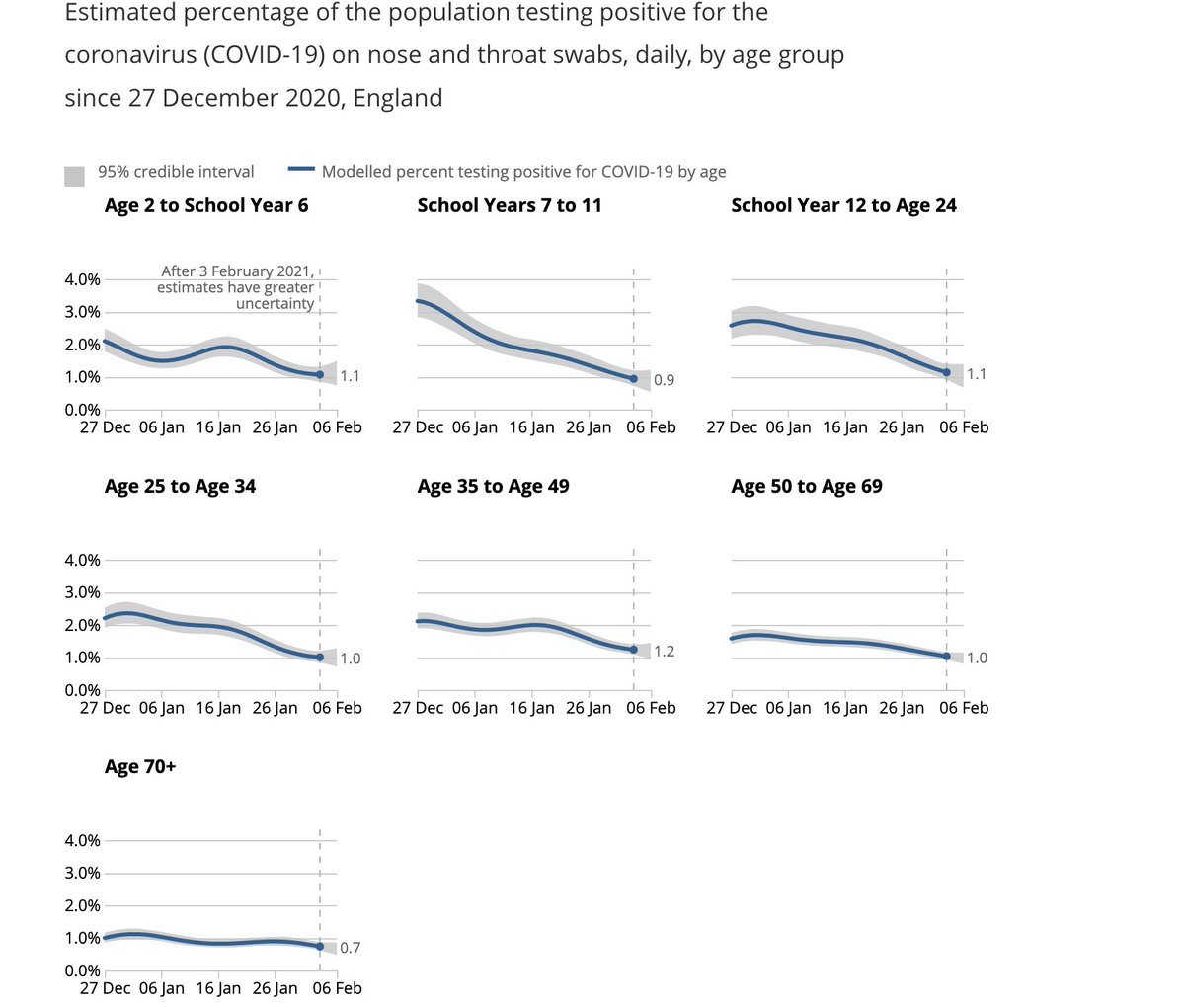
We see steep drops in both primary & secondary school groups after end of term (18th December), but these drops plateau out in primary school children, where attendance has been >20% after re-opening in January (by contrast with 2ndary schools where this is ~5%).
I've heard a lot of scientists claim these three - including most recently the chief advisor to the CDC, where the claim that most transmission doesn't happen within the walls of schools. There is strong evidence to rebut this claim. Let's look at
The science shows us that most disease transmission does not happen in the walls of the school, but it comes in from the community. So, CDC is advocating to get our K-5 students back in school at least in a hybrid mode with universal mask wearing and 6 ft of distancing. https://t.co/dfvJ2nl2s4
— Rochelle Walensky, MD, MPH (@CDCDirector) February 14, 2021
Let's look at the trends of infection in different age groups in England first- as reported by the ONS. Being a random survey of infection in the community, this doesn't suffer from the biases of symptom-based testing, particularly important in children who are often asymptomatic
A few things to note:
1. The infection rates among primary & secondary school children closely follow school openings, closures & levels of attendance. E.g. We see a dip in infections following Oct half-term, followed by a rise after school reopening.
We see steep drops in both primary & secondary school groups after end of term (18th December), but these drops plateau out in primary school children, where attendance has been >20% after re-opening in January (by contrast with 2ndary schools where this is ~5%).
More from Government

🧵⬇️1. Fb is LifeLog, LifeLog is Darpa, and DARPA is a Enterprise Run by CIA... Well... Past President... Big Tech, Big Pharma, MSM, HOLLYWOOD, DC...
Past Presidents....Zuckerberg, Gates...
All C_A... the Family business.... The company...
2. Past Presidents....Zuckerberg, Gates...
All C_A... the Family business.... The company...The Farm.... all C_A assets... most of them related by blood, business, or marriage...

3. "The individual is handicapped by coming face-to-face with a conspiracy so monstrous he cannot believe it exists. The American mind simply has not come to a realization of the evil which has been introduced into our midst." - J. Edgar Hoover

4. diff. names & faces.... Monsters that lurk in the Shadows. Swamp, Deep State, Establishment, Globalist Elite Cabal...
Shall we go back...How far back...

5. I know these monsters... it's when I try to explain them to others is when I run into a problem.This is why I'm better at retweeting and compiling. I never know where to start... Everytime I try to thread, i end up w/ a messy monstrous web.I'm better at helping others thread.

Past Presidents....Zuckerberg, Gates...
All C_A... the Family business.... The company...
BREAKING\u2014 \u201cThis \u2018SHADOW GOVERNMENT\u2019 had a huge hand in running the show on Nov. 3 and you may have not known it\u201d says attorney Phil Kine. @newsmax pic.twitter.com/8ypASTEA1Z
— White Rabbit News \u277c (@WhiteRabbitNN) December 17, 2020
2. Past Presidents....Zuckerberg, Gates...
All C_A... the Family business.... The company...The Farm.... all C_A assets... most of them related by blood, business, or marriage...
3. "The individual is handicapped by coming face-to-face with a conspiracy so monstrous he cannot believe it exists. The American mind simply has not come to a realization of the evil which has been introduced into our midst." - J. Edgar Hoover
4. diff. names & faces.... Monsters that lurk in the Shadows. Swamp, Deep State, Establishment, Globalist Elite Cabal...
Shall we go back...How far back...
5. I know these monsters... it's when I try to explain them to others is when I run into a problem.This is why I'm better at retweeting and compiling. I never know where to start... Everytime I try to thread, i end up w/ a messy monstrous web.I'm better at helping others thread.




Typically excellent piece from @dsquareddigest The exponential insight is especially neat. Think of it a little like fishing...today you can’t export oysters to the EU (because you simply aren’t allowed to), tomorrow you don’t have a fish exporting business (to the EU).
The extremely small minority of people who known anything about this who think that Brexit will be good for the City make a number of arguments which I shall address in turn...
1. They need us more than we need them. This is a variant of the German carmakers argument. And we know how that went...Business will follow the profit opportunity and if that has moved then so will the business...
And what do we mean by us / we. We’re not talking about massed ranks of Euro investing / trading etc blue blooded British institutions.
Au contraire. We’re talking about the London based subs of US, Asian and indeed European capital markets players...As soon as they think the profit opportunity has moved then so will they...it’s a market innit...
London's status as a financial centre isn't as secure as some might think | Dan Davies https://t.co/q9SU7ra4oF
— The Guardian (@guardian) February 13, 2021
The extremely small minority of people who known anything about this who think that Brexit will be good for the City make a number of arguments which I shall address in turn...
1. They need us more than we need them. This is a variant of the German carmakers argument. And we know how that went...Business will follow the profit opportunity and if that has moved then so will the business...
And what do we mean by us / we. We’re not talking about massed ranks of Euro investing / trading etc blue blooded British institutions.
Au contraire. We’re talking about the London based subs of US, Asian and indeed European capital markets players...As soon as they think the profit opportunity has moved then so will they...it’s a market innit...
You May Also Like





Funny, before the election I recall lefties muttering the caravan must have been a Trump setup because it made the open borders crowd look so bad. Why would the pro-migrant crowd engineer a crisis that played into Trump's hands? THIS is why. THESE are the "optics" they wanted.
This media manipulation effort was inspired by the success of the "kids in cages" freakout, a 100% Stalinist propaganda drive that required people to forget about Obama putting migrant children in cells. It worked, so now they want pics of Trump "gassing children on the border."
There's a heavy air of Pallywood around the whole thing as well. If the Palestinians can stage huge theatrical performances of victimhood with the willing cooperation of Western media, why shouldn't the migrant caravan organizers expect the same?
It's business as usual for Anarchy, Inc. - the worldwide shredding of national sovereignty to increase the power of transnational organizations and left-wing ideology. Many in the media are true believers. Others just cannot resist the narrative of "change" and "social justice."
The product sold by Anarchy, Inc. is victimhood. It always boils down to the same formula: once the existing order can be painted as oppressors and children as their victims, chaos wins and order loses. Look at the lefties shrieking in unison about "Trump gassing children" today.
Funny there are those who think these migrant caravans were a FANTASTIC idea that's going to take the immigration issue away from you.
— Brian Cates (@drawandstrike) November 26, 2018
Like several weeks watching a rampaging horde storm the fences & throw rocks at our border patrol agents & getting gassed = great optics!
This media manipulation effort was inspired by the success of the "kids in cages" freakout, a 100% Stalinist propaganda drive that required people to forget about Obama putting migrant children in cells. It worked, so now they want pics of Trump "gassing children on the border."
There's a heavy air of Pallywood around the whole thing as well. If the Palestinians can stage huge theatrical performances of victimhood with the willing cooperation of Western media, why shouldn't the migrant caravan organizers expect the same?
It's business as usual for Anarchy, Inc. - the worldwide shredding of national sovereignty to increase the power of transnational organizations and left-wing ideology. Many in the media are true believers. Others just cannot resist the narrative of "change" and "social justice."
The product sold by Anarchy, Inc. is victimhood. It always boils down to the same formula: once the existing order can be painted as oppressors and children as their victims, chaos wins and order loses. Look at the lefties shrieking in unison about "Trump gassing children" today.





