
Another thread so soon? This one's going to be about a classic argument, sex determination. There are five methods of sex determination and I'm going to go into depth on my arguments on why I state that sex is able to be determined in all cases. #intersex
The five determination methods in question:
Karyotype, Presenting Genitalia, Gonads, Hormone Production, Internal Reproductive Structures.
XX, XY. The point is, humans can only possibly have either a X and Y in their karyotype. However a Y monosomy isn't possible, at least not survivable anyways. The X also comes before the Y as well, but there's more to this particular determination.
Hopefully karyotype is explained now..
To start we'll go into how there's different types of gonads and it is possible for a body to have two of the types, especially in that 0.02% of intersex people. In that case you classify by which one is functional.
External genitalia is pretty obvious in regards to having a clitoris or a penis. A vagina, or no vagina. However like I said there are some exceptions.
Reproductive structures are what we're referring to when we talk to Mullerian and Wolffian structures.
That said, PMDS would either be marked as both for this or male due to functional Wolffian.
More from Society

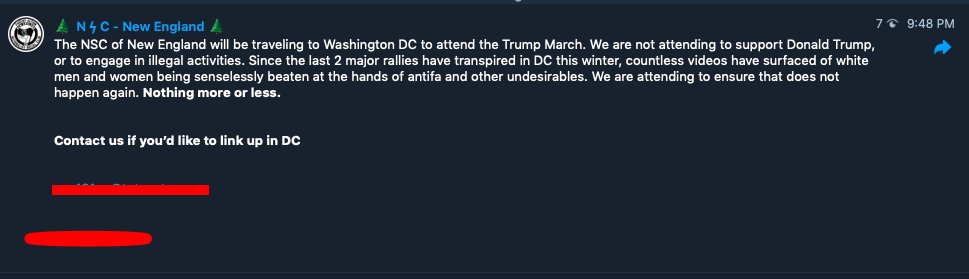
Tomorrow, January 6th, MAGA chuds, Proud Boys, and white supremacists are planned to descend on Washington D.C. to contest the election. Among them will be NSC-131, a New England based neo-Nazi organization. Let's welcome them by saying hi to one of their members, Eddie Stuart!
Edward Stuart, from Chester, New Hampshire, has been a member of Nationalist Social Club (NSC) since the very beginning and is a staple participant in their actions. He is known in NSC chats as "Carl Jung" and is well connected in the New England Nazi scene.
2/
NSC-131 is a neo-Nazi group that was started in Massachusetts in early 2020 by Chris Hood. You can learn more about NSC and it's members in these threads:
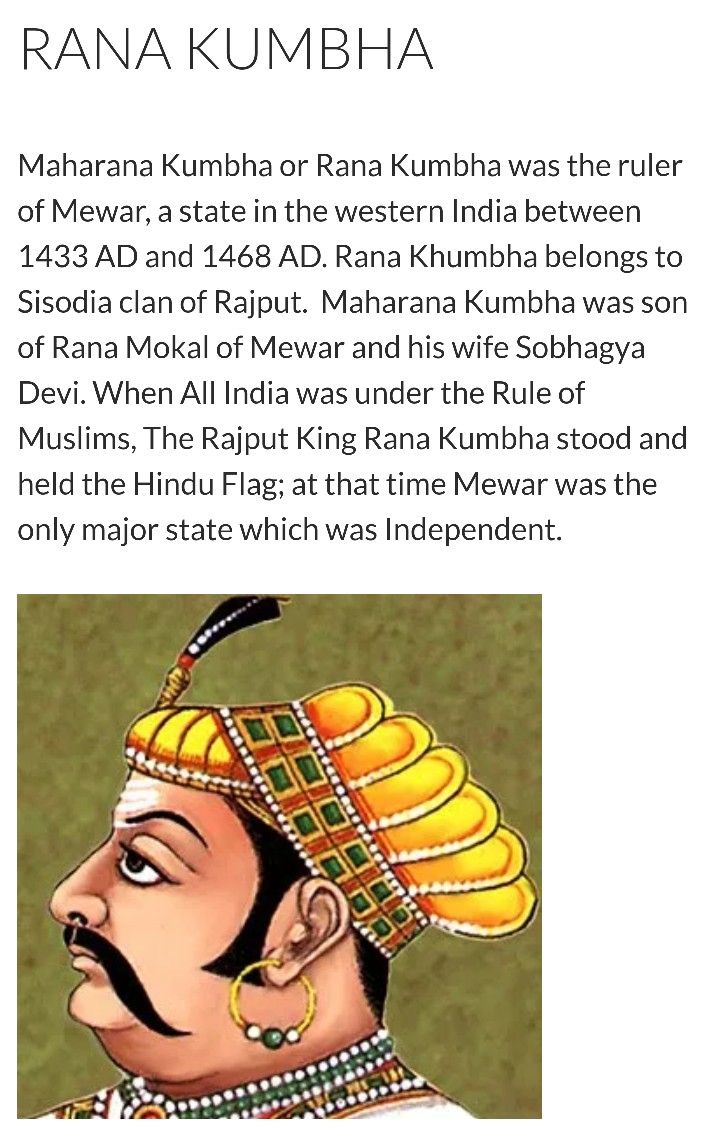
Eddie describes his ideology as "Esoteric Hitlerism" which is an occult form of Nazism that literally worships Adolf Hitler as a god, or, specifically, as an incarnation of the Hindu God Vishnu. Here is Ed holding the RigVeda with some of his occult Nazi pals. Interesting Ed!
4/

Much of this ideological insight was gained from Eddie's Twitter, where he originally used his "Carl Jung" persona and reposts explicit neo-fascist content and racist memes. In one edited picture, Eddie can be seen at an NSC event in late June 2020 holding a Nazi Sonnenrad flag
5

Edward Stuart, from Chester, New Hampshire, has been a member of Nationalist Social Club (NSC) since the very beginning and is a staple participant in their actions. He is known in NSC chats as "Carl Jung" and is well connected in the New England Nazi scene.
2/
NSC-131 is a neo-Nazi group that was started in Massachusetts in early 2020 by Chris Hood. You can learn more about NSC and it's members in these threads:
1/ Let\u2019s talk about a III%er turned Proud Boy turned Resist Marxism turned Patriot Front turned The Base affiliate.
— AntiFash Gordon (@AntiFashGordon) April 10, 2020
He now runs a new crew, the National Socialist Club, based on football hooliganism.\u2070\u2070
Some of you already know him.\u2070\u2070
His name is Chris Hood, of Boston, MA. pic.twitter.com/nXAxWugHcu
Eddie describes his ideology as "Esoteric Hitlerism" which is an occult form of Nazism that literally worships Adolf Hitler as a god, or, specifically, as an incarnation of the Hindu God Vishnu. Here is Ed holding the RigVeda with some of his occult Nazi pals. Interesting Ed!
4/
Much of this ideological insight was gained from Eddie's Twitter, where he originally used his "Carl Jung" persona and reposts explicit neo-fascist content and racist memes. In one edited picture, Eddie can be seen at an NSC event in late June 2020 holding a Nazi Sonnenrad flag
5



You May Also Like









Trump is gonna let the Mueller investigation end all on it's own. It's obvious. All the hysteria of the past 2 weeks about his supposed impending firing of Mueller was a distraction. He was never going to fire Mueller and he's not going to
Mueller's officially end his investigation all on his own and he's gonna say he found no evidence of Trump campaign/Russian collusion during the 2016 election.
Democrats & DNC Media are going to LITERALLY have nothing coherent to say in response to that.
Mueller's team was 100% partisan.
That's why it's brilliant. NOBODY will be able to claim this team of partisan Democrats didn't go the EXTRA 20 MILES looking for ANY evidence they could find of Trump campaign/Russian collusion during the 2016 election
They looked high.
They looked low.
They looked underneath every rock, behind every tree, into every bush.
And they found...NOTHING.
Those saying Mueller will file obstruction charges against Trump: laughable.
What documents did Trump tell the Mueller team it couldn't have? What witnesses were withheld and never interviewed?
THERE WEREN'T ANY.
Mueller got full 100% cooperation as the record will show.
BREAKING: President Donald Trump has submitted his answers to questions from special counsel Robert Mueller
— Ryan Saavedra (@RealSaavedra) November 20, 2018
Mueller's officially end his investigation all on his own and he's gonna say he found no evidence of Trump campaign/Russian collusion during the 2016 election.
Democrats & DNC Media are going to LITERALLY have nothing coherent to say in response to that.
Mueller's team was 100% partisan.
That's why it's brilliant. NOBODY will be able to claim this team of partisan Democrats didn't go the EXTRA 20 MILES looking for ANY evidence they could find of Trump campaign/Russian collusion during the 2016 election
They looked high.
They looked low.
They looked underneath every rock, behind every tree, into every bush.
And they found...NOTHING.
Those saying Mueller will file obstruction charges against Trump: laughable.
What documents did Trump tell the Mueller team it couldn't have? What witnesses were withheld and never interviewed?
THERE WEREN'T ANY.
Mueller got full 100% cooperation as the record will show.
