ECTOPIC PREGNANCY
A woman just lost her life due to ectopic pregnancy!
It's a pregnancy in which the embryo attaches outside the womb. It can be life-threatening.
But we can save lives by helping educate women on our Timelines with this.
THREAD 🧵
In the human body, a fertilized egg hardly survives outside the womb. If allowed to grow, it may damage nearby organs & cause severe blood loss.
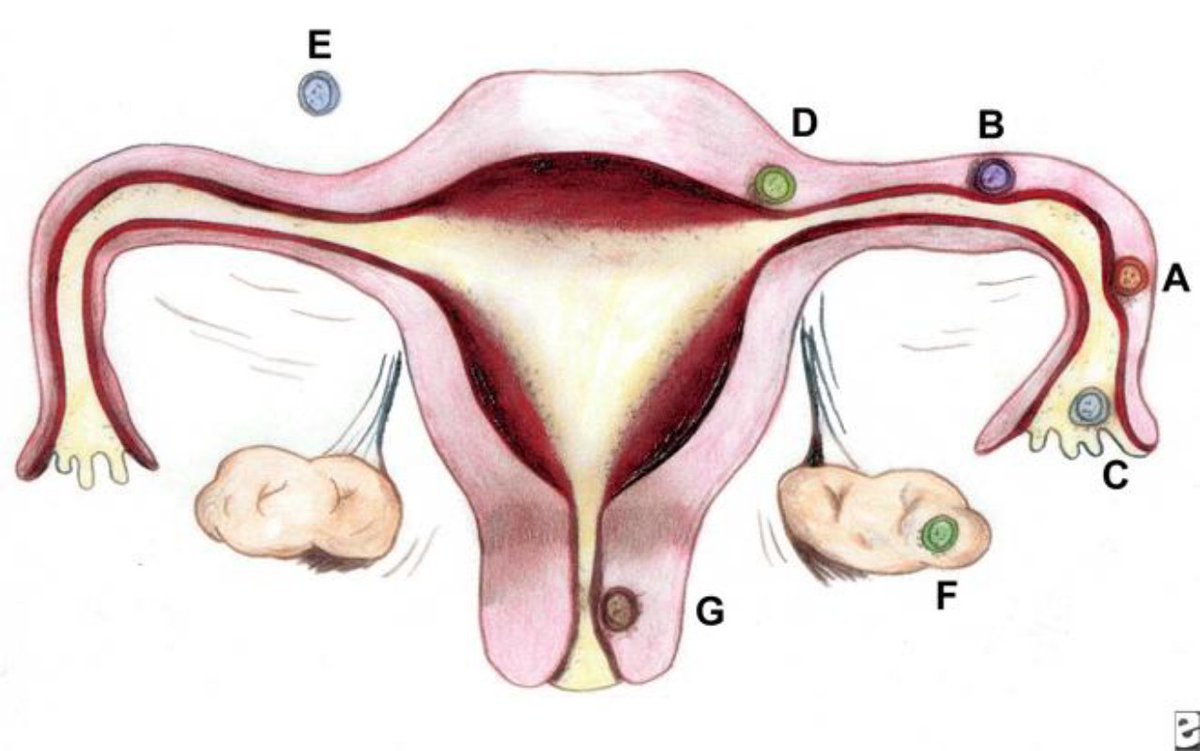
The bulk of ectopic pregnancies occur in/along the Fallopian tubes.
Some in the ovaries, cervix or a random location in the abdomen.
The usual symptoms of ectopic pregnancy a woman may experience esp. in early pregnancy are;
* Abdominal pain
* Vaginal bleeding, &
* Amenorrhea (missing your period)
Other pregnancy symptoms like breast fullness & occasional nausea may be there too.
But the common DANGER SIGNS of ectopic pregnancy that may signify rupture are;
🔴 Rigid abdomen
🔴 Severe abdominal pain
🔴 Shoulder tip pain, &
🔴 Signs of shock such as cold hands & feet.
With these signs, immediate medical attention is needed to save the woman's life!
Your chances of having an ectopic pregnancy are higher if you have;
1. Previous ectopic pregnancy
2. STI's like gonorrhea
3. Fertility treatments like IVF*
4. Fallopian tube surgeries
5. Pregnancy while using an Intrauterine Contraceptive Device
6. Smoking history! 🚭