As expected, many participants reported stress, anxiety, and depression. But the study also looked into *what* exactly made participants feel distressed.
https://t.co/ZHCbh10pBG
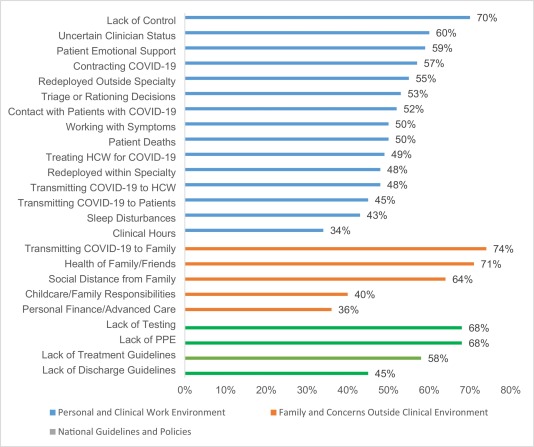
This graph is showing % of participants who found these factors "highly distressing." Note in the work environment section (blue) the number of things that rank higher than patient deaths.
These include:
- Perceptions of a lack of control and/or uncertainty
- Performing clinical work that is outside of your specialty
- The need/expectation for healthcare providers to provide social support to patients in lieu of their families (due to visitation restrictions)
- Difficult triage decisions or rationing of care (potential or actual) due to resource scarcity
- And also fears related to getting/transmitting Covid within the work environment - in particular, the uncertain Covid status of other healthcare providers
I bring this up because I think there are some good lessons here from Wave 1 for hospital leaders facing Wave 3.
First, if the #1 source of distress is loss of control and uncertainty, than people need as much control and certainty as possible. Transparency, minimal bullshit, problems stated clearly and promptly. More information is better.
Whenever possible, decisions should be made after engagement of multiple stakeholders, and with opportunity for feedback and changing course. We didn't always have time for that in Wave 1. But we had intervening months to learn better approaches in the period since.
Examples of pediatricians seeing adults, radiologists deployed to the ICU have been thrown out there as a signal for hospital system overload. I don't think we have really stopped to acknowledge how distressing it is to be asked to practice outside of your usual scope of work.
Hospital leadership needs to treat this like the very big deal it is, and provide concrete support for rapid skill development and psychological distress beyond "please watch these YouTube videos, phone a friend, you'll be fine."
HCWs at this point should know the range of resources they have to support patients who are isolated from their loved ones and also the processes and bodies that support triage / ethical decision-making in the setting of scarce resources.
But if they do not exist, if they are not sufficient, or if they are not sufficiently communicated, this needs to happen ASAP.
There are two other things I'd point out from the study. First, note how low the clinical hours worked was on the "highly distressed" chart. It's a concern, for sure, but not the main thing. I suspect it's more of an issue at this point in the pandemic...
...when people are exhausted in every sense. But I also think that this is something we amply talk about, because it's familiar and we know how to talk about it. I've gotten my share of "we know this sucks but it's what we gotta do for x reasons, here comes second back-up" ...
And I wonder if there's less severe distress because leadership tends to talk about it clearly and plainly and without the vagueness, avoidance, or insincerity that seems to be used around other topics (like PPE use, or practicing out of specialty, or triage decisions).
The other thing from the study is >60% of participants reported feeling a high level of purpose and meaning. I think of this a lot. Because that's something HCWs bring to the table, an asset that is in some ways hospitals' to keep or lose.
And I think the way you eff that up is actually related to all of the above. When employees are treated like children rather than trusted and respected partners in the work, when they are subjected to unsafe situations without a good faith effort to fix them...
Cheery declarations of "remember, we're all in this together" or wellness Zooms or downloadable apps have no hope to sustain morale.
Once again, I have spoken.