
Just a one hour shift in my sleep schedule can screw me up for days. 2/16
Okay, let's start this hypersomnia thread!
[note - I am not looking for unsolicited advice.]
Idiopathic hypersomnia or narcolepsy (not the same, but similar) is very hard to describe to people.
When I say "I slept 10 hours last night and I'm still tired" I'm not bragging. 1/16
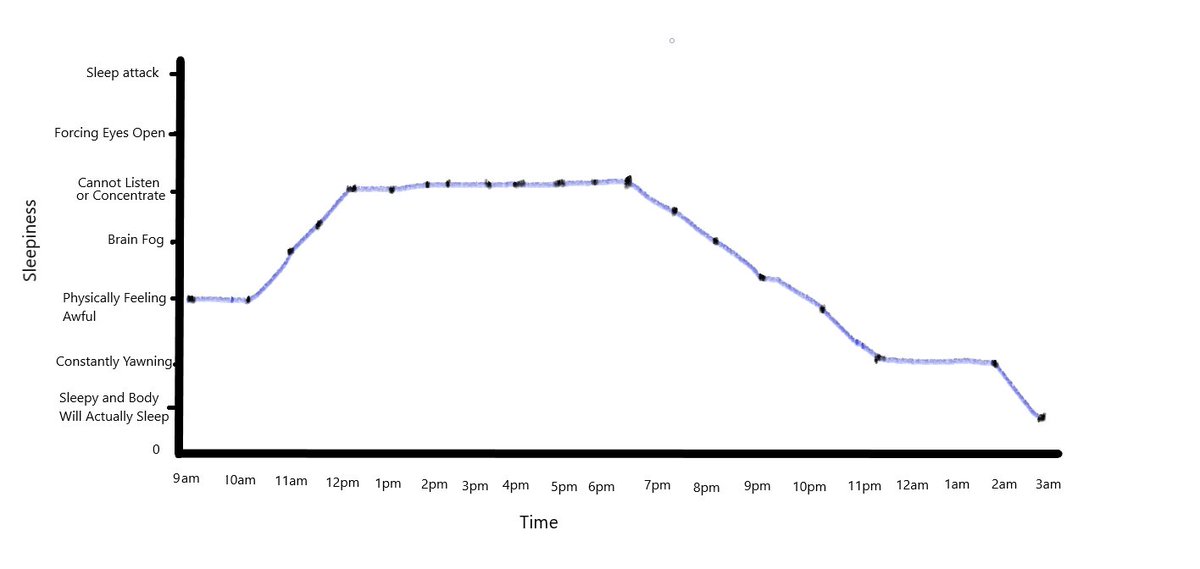
Just a one hour shift in my sleep schedule can screw me up for days. 2/16
I'm going to show you ways this happens. I can usually withstand 1 day of waking up early, with some consequences, but 2 days in a row kills me. 4/16
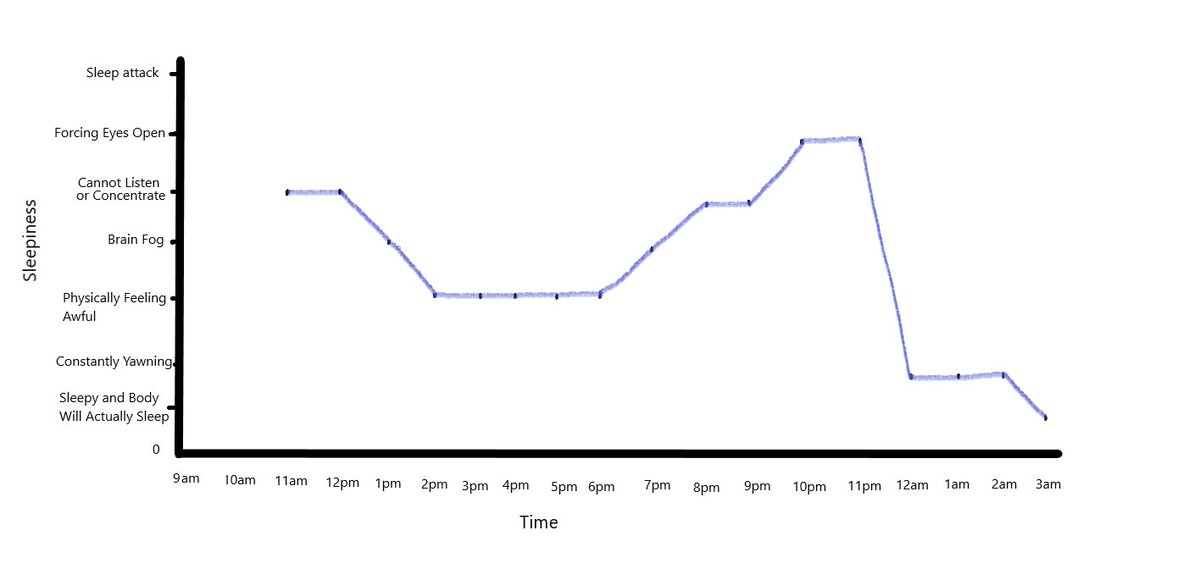
This is when I can sleep in until 11am because I do not have an event the next day. My body is not happy because of my switch in sleep cycles. It's not great, but it's not completely terrible. 6/16
More from Health






Let's talk honestly about "informed consent."
Someone with decades of training gives someone with none advice usually packed into 1-3 mins. Huge amount is based on trust. Huge potential for bias built in. But also there is no obligation to provide real alternative options.
I am classified as 'gifted' (obnoxious and ableist term). I mention because of what I am about to say. You all know that I was an ambulatory wheelchair user previously - could stand - but contractures have ended that. When I pleaded for physio, turned down. But did you know...
I recently was chatting with a doctor I know and explaining what happened and the day the physiatrist told me it was too late and nothing could be done. The doctor asked if I'd like one of her friends/colleagues to give second opinion. I said yes please! So...
She said can you send me MRI and other imaging they did to determine it wasn't possible to address your contractures.
Me: What?
Dr.: They did a MRI first before deciding right?
Me: No
Dr: What did they do??!
Me: Examined me for 2 minutes.
Dr: I am very angry rn. Can't talk.
My point is you don't even know if you are making "informed" decisions because the only source of information you have is the person who has already decided what they think you should do. And may I remind you of a word called 'compliance.'
Someone with decades of training gives someone with none advice usually packed into 1-3 mins. Huge amount is based on trust. Huge potential for bias built in. But also there is no obligation to provide real alternative options.
MAiD isn't eugenics. The task for the medical profession is to ensure informed consent. Failures on that front should result in enforcement of the law. But Bill C-7 is the result of the existing regime imposing unnecessary, unconstitutional harms by blocked access to MAiD.
— Emmett Macfarlane (@EmmMacfarlane) February 13, 2021
I am classified as 'gifted' (obnoxious and ableist term). I mention because of what I am about to say. You all know that I was an ambulatory wheelchair user previously - could stand - but contractures have ended that. When I pleaded for physio, turned down. But did you know...
I recently was chatting with a doctor I know and explaining what happened and the day the physiatrist told me it was too late and nothing could be done. The doctor asked if I'd like one of her friends/colleagues to give second opinion. I said yes please! So...
She said can you send me MRI and other imaging they did to determine it wasn't possible to address your contractures.
Me: What?
Dr.: They did a MRI first before deciding right?
Me: No
Dr: What did they do??!
Me: Examined me for 2 minutes.
Dr: I am very angry rn. Can't talk.
My point is you don't even know if you are making "informed" decisions because the only source of information you have is the person who has already decided what they think you should do. And may I remind you of a word called 'compliance.'
You May Also Like




1/ 👋 Excited to share what we’ve been building at https://t.co/GOQJ7LjQ2t + we are going to tweetstorm our progress every week!
Week 1 highlights: getting shortlisted for YC W2019🤞, acquiring a premium domain💰, meeting Substack's @hamishmckenzie and Stripe CEO @patrickc 🤩
2/ So what is Brew?
brew / bru : / to make (beer, coffee etc.) / verb: begin to develop 🌱
A place for you to enjoy premium content while supporting your favorite creators. Sort of like a ‘Consumer-facing Patreon’ cc @jackconte
(we’re still working on the pitch)
3/ So, why be so transparent? Two words: launch strategy.
jk 😅 a) I loooove doing something consistently for a long period of time b) limited downside and infinite upside (feedback, accountability, reach).
cc @altimor, @pmarca
4/ https://t.co/GOQJ7LjQ2t domain 🍻
It started with a cold email. Guess what? He was using BuyMeACoffee on his blog, and was excited to hear about what we're building next. Within 2w, we signed the deal at @Escrowcom's SF office. You’re a pleasure to work with @MichaelCyger!
5/ @ycombinator's invite for the in-person interview arrived that evening. Quite a day!
Thanks @patio11 for the thoughtful feedback on our YC application, and @gabhubert for your directions on positioning the product — set the tone for our pitch!
Week 1 highlights: getting shortlisted for YC W2019🤞, acquiring a premium domain💰, meeting Substack's @hamishmckenzie and Stripe CEO @patrickc 🤩
2/ So what is Brew?
brew / bru : / to make (beer, coffee etc.) / verb: begin to develop 🌱
A place for you to enjoy premium content while supporting your favorite creators. Sort of like a ‘Consumer-facing Patreon’ cc @jackconte
(we’re still working on the pitch)
3/ So, why be so transparent? Two words: launch strategy.
jk 😅 a) I loooove doing something consistently for a long period of time b) limited downside and infinite upside (feedback, accountability, reach).
cc @altimor, @pmarca
4/ https://t.co/GOQJ7LjQ2t domain 🍻
It started with a cold email. Guess what? He was using BuyMeACoffee on his blog, and was excited to hear about what we're building next. Within 2w, we signed the deal at @Escrowcom's SF office. You’re a pleasure to work with @MichaelCyger!
5/ @ycombinator's invite for the in-person interview arrived that evening. Quite a day!
Thanks @patio11 for the thoughtful feedback on our YC application, and @gabhubert for your directions on positioning the product — set the tone for our pitch!

To people who are under the impression that you can get rich quickly by working on an app, here are the stats for https://t.co/az8F12pf02
📈 ~12000 vistis
☑️ 109 transactions
💰 353€ profit (285 after tax)
I have spent 1.5 months on this app. You can make more $ in 2 days.
🤷♂️

I'm still happy that I launched a paid app bcs it involved extra work:
- backend for processing payments (+ permissions, webhooks, etc)
- integration with payment processor
- UI for license activation in Electron
- machine activation limit
- autoupdates
- mailgun emails
etc.
These things seemed super scary at first. I always thought it was way too much work and something would break. But I'm glad I persisted. So far the only problem I have is that mailgun is not delivering the license keys to certain domains like https://t.co/6Bqn0FUYXo etc. 👌
omg I just realized that me . com is an Apple domain, of course something wouldn't work with these dicks
📈 ~12000 vistis
☑️ 109 transactions
💰 353€ profit (285 after tax)
I have spent 1.5 months on this app. You can make more $ in 2 days.
🤷♂️
I'm still happy that I launched a paid app bcs it involved extra work:
- backend for processing payments (+ permissions, webhooks, etc)
- integration with payment processor
- UI for license activation in Electron
- machine activation limit
- autoupdates
- mailgun emails
etc.
These things seemed super scary at first. I always thought it was way too much work and something would break. But I'm glad I persisted. So far the only problem I have is that mailgun is not delivering the license keys to certain domains like https://t.co/6Bqn0FUYXo etc. 👌
omg I just realized that me . com is an Apple domain, of course something wouldn't work with these dicks




