Consider the possibility that all our naso-pharynxes together make up a single ecosystem, in which only one predator can be completely dominant.
We are not saying that this has definitely happened with Covid - but it would explain the disappearance of flu this year.
Every winter, we see "excess deaths" in the sense that more (mainly elderly) people die in the winter than in the summer.
This is a worldwide phenomenon.
It is now thought that all or nearly all of the extra deaths in Winter are due to infection with winter respiratory viruses, mainly influenza:
https://t.co/xOHDcSRgGB
However, we do not - and never have - extensively tested for the presence of such viruses in the critically ill elderly population, so we really have no idea how frequently infection is present, or in fact what its contribution to death is.
In 2017, researchers at 2 morgues in Spain swab-tested a series of recently deceased elderly individuals and found respiratory viruses in 47% of them. In only 15% of these had a diagnosis been made prior to death.
https://t.co/PBUnIfLtaf
The death certificates for all these individuals featured the usual wide range of pathologies that would be expected in this age group, but viruses were detected (post-mortem) across all categories of causes of death.
For this cohort - presumably representative of similar cohorts of subjects across Europe - what would the mortality picture have looked like had we applied a policy of recording the detected respiratory virus as the cause of death, irrespective of other pathologies?
That is, in effect, what we might be doing now, to some extent - Covid taking the place of other viruses (particularly influenza).
In other words, might some of the Covid deaths we are now seeing be those that would have sadly died in a normal winter anyway?
As is usually the case, the picture is more complex and there are probably a number of other factors contributing to the current mortality picture.
Firstly, there will of course be some additional "pure Covid" deaths as the virus moves into its endemic rather than pandemic stage.
This was seen in the year following the Swine flu pandemic:
https://t.co/uIB5lF7CKU
Secondly, there is increasing evidence of deaths being caused by nearly a year of restricted access to healthcare.
In fact, given the nation's state of health and presence of multiple diseases, it would be more surprising if there was no such effect.
That attendances at A&E departments making up the Syndromic Surveillance System (currently covering 82 hospitals in England) are running below the same period last year is consistent with this:
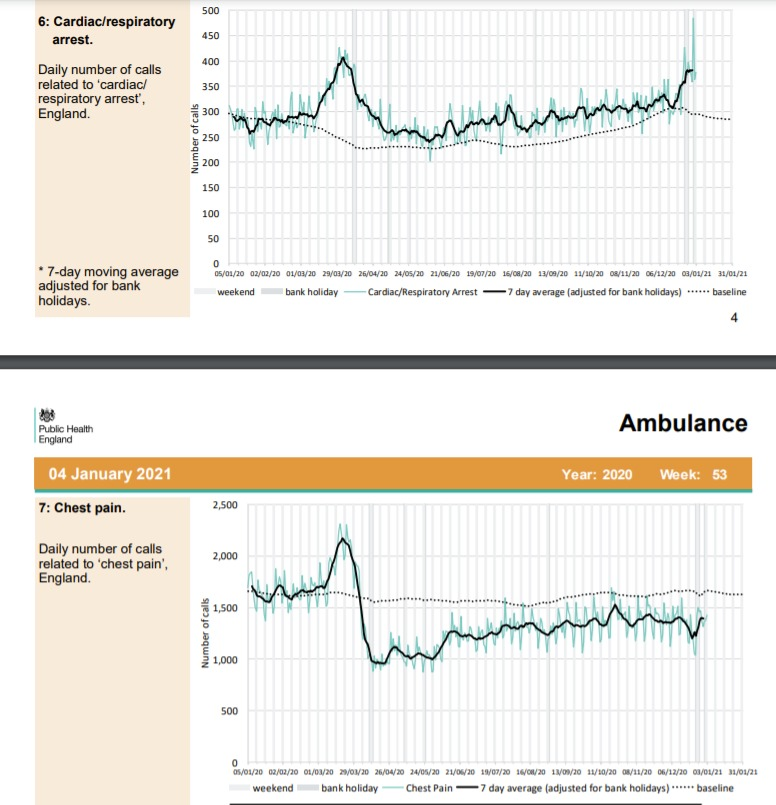
Ambulance calls for cardiac/respiratory arrest calls are high, yet calls for chest pain appear to be lower than average.
This is worryingly consistent with a picture of reluctance to seek help in time.
This would be highly unlikely to result in no excess deaths.
The numbers involved are not small, the arrest calls appear to be ~50-75 more than expected (daily), but chest pain calls ~250 per day fewer than expected.
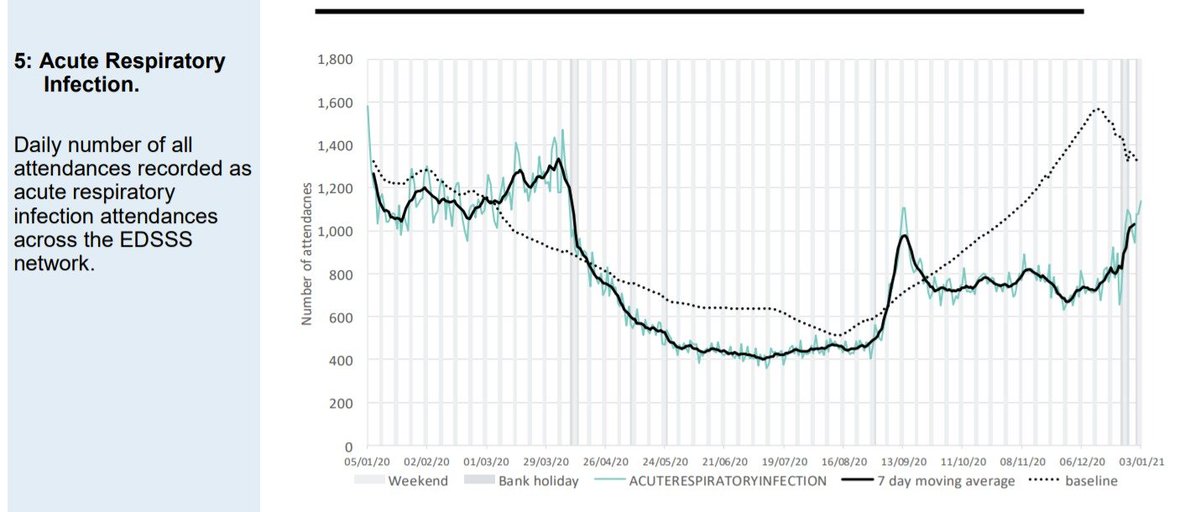
Surprisingly, attendances for acute respiratory infections are well below average for the entire Autumn and Winter so far; although rising recently they are still below average.
This is consistent with the point made above - ie could Covid be replacing flu this year?
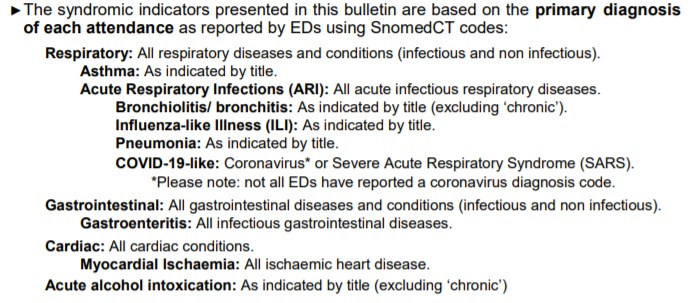
Some have previously claimed that this category does not include Covid, but the notes in the report seem quite clear that it does.
Finally, it must be acknowledged that the emergence of Covid is currently causing significant strain on our NHS, although it is worthwhile acknowledging that several reasons must contribute to this.
Firstly, it appears that treating Covid patients is more complex and onerous than treating those who would previously have been patients with a variety of other
- mainly undiagnosed - respiratory viruses.
Secondly, the reduction in beds available for a growing and ageing population is a major problem; they fell from 240,000 in 2000 to under 165,000 in 2019.
The figure fell by a further 10,000 beds to allow for social distancing between patients in hospital.
The need to segregate suspected Covid from confirmed Covid and non-Covid patients has a detrimental effect of bed management, as does the need for smaller bay sizes to accommodate distancing.
A&E departments can easily become clogged up by delays in finding beds for patients.
In some hospitals patients are not being discharged until their Covid test returns as negative.
Clearly returning patients to care homes during the window of infectivity would be a bad idea.
Beyond that this policy is surely inadvisable.
It should be recalled that some patients continue to test PCR positive for weeks or even months after infection, as experienced by the unfortunate British students stuck in Italy last summer:
https://t.co/qaIsjDD5Mm
PCR testing has led to a staffing crisis, as asymptomatic staff - even those who must be immune through known prior exposure - are made to self-isolate for two weeks.
50,000 NHS staff are absent for Covid reasons, out of 100,000 total absences.
https://t.co/qgpc00Otie
Finally, it should be acknowledged that staff are having to work in PPE and change it frequently, adding a significant additional burden to an already heavy workload.