
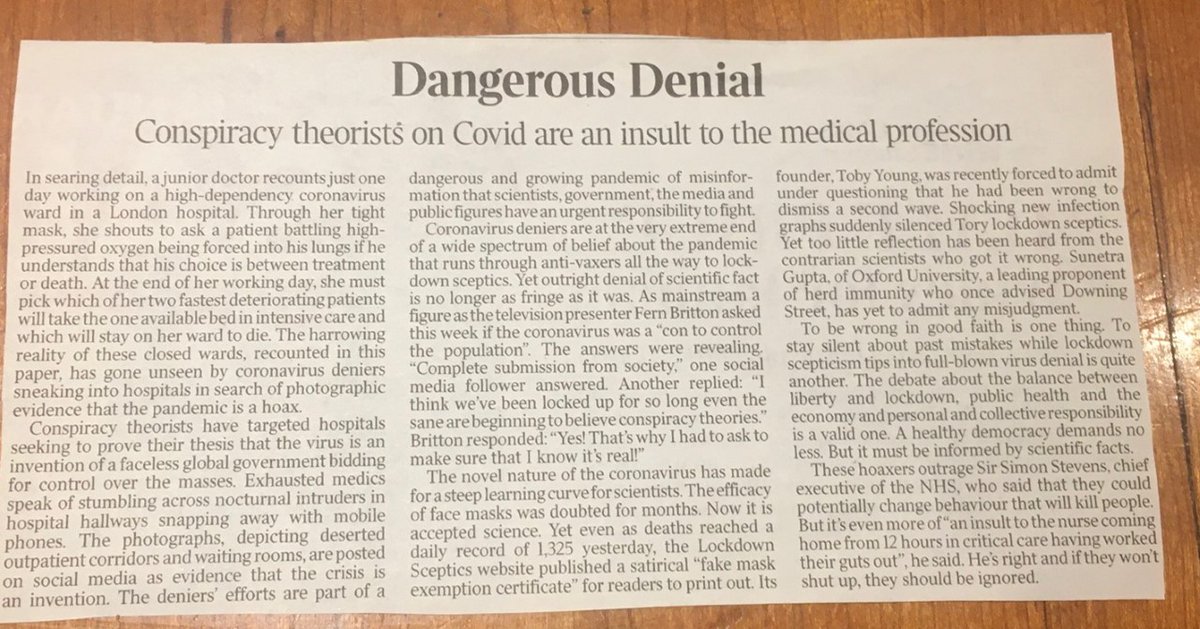
1/42 Good to see yesterday’s @thetimes editorial attacking the pandemic of covid misinformation. Here’s my twitter contribution to fighting it, as suggested. Lockdown and covid sceptics continue to consistently misuse cherry picked data to argue NHS not unusually busy.
26/42 Are there any national datasets that accurately capture what is going on? The brilliant @jburnmurdoch has highlighted number of admissions into ICU. The message from his animated chart (click on link) couldn\u2019t be clearer \u2013 this winter is v unusual: https://t.co/76ZvHU2pmV. pic.twitter.com/tu99YmS5TI
— Chris Hopson (@ChrisCEOHopson) January 10, 2021
More from News


1/1 On @seanhannity last night (at 5:56 of this clip), @SenTedCruz said that the Hayes-Tilden Commission was "charged with reviewing the evidence and making a determination about the disputed ballots." That's incorrect. The Commission was tasked with determining which rival ...
2/2 ... group of electors was appointed by the authority within state government entitled to make that appointment at the time the electors cast their votes on the constitutionally required day. Justice Joseph Bradley, who was held the intentionally tiebreaking seat on the ...
3/3 ... 15-member Commission, explained his decision in favor of Hayes by saying that it was NOT the Commission's authority (NOR Congress's, from which the Commission derived its subsidiary power) to determine whether the state properly counted its popular vote. Instead, ...
4/4 ...it was the Commission's job to figure out which of the competing claims was correct concerning who had authority under state law to make the determination upon which the appointment of electors would be based. For Florida, Bradley ruled that the state's canvassing board...
5/5... had this authority at the time the electors voted & thus Congress was obligated to accept the votes cast by the electors that the canvassing board had appointed, and this was true even if the canvassing board's appointment was based on a mistake or even fraud affecting ...
Tomorrow is an important day. We have an obligation to protect the integrity of the election & our democratic system. That\u2019s why 10 of my colleagues & I are calling for an Electoral Commission to conduct an emergency 10-day audit to examine voter fraud allegations. pic.twitter.com/fExTpxlmKl
— Senator Ted Cruz (@SenTedCruz) January 6, 2021
2/2 ... group of electors was appointed by the authority within state government entitled to make that appointment at the time the electors cast their votes on the constitutionally required day. Justice Joseph Bradley, who was held the intentionally tiebreaking seat on the ...
3/3 ... 15-member Commission, explained his decision in favor of Hayes by saying that it was NOT the Commission's authority (NOR Congress's, from which the Commission derived its subsidiary power) to determine whether the state properly counted its popular vote. Instead, ...
4/4 ...it was the Commission's job to figure out which of the competing claims was correct concerning who had authority under state law to make the determination upon which the appointment of electors would be based. For Florida, Bradley ruled that the state's canvassing board...
5/5... had this authority at the time the electors voted & thus Congress was obligated to accept the votes cast by the electors that the canvassing board had appointed, and this was true even if the canvassing board's appointment was based on a mistake or even fraud affecting ...

Durham County Council has upheld my complaint that Councillor David Boyes breached its Code of Conduct for communications in respect of Travellers. This would appear to be the first time in England that a councillor has been so held to account for such communications. [1/16]
The grounds for the complaint are already set out by me: https://t.co/0MDqO6dyja. In summary: on 7 May 2020, Cllr Boyes posted on a Facebook site he shared with another councillor a video of scorch damage from barbeque trays and littering on and around a picnic table.
[2/16]
The table was in a picnic area in a nature reserve in the Easington constituency which Cllr Boyes represents. The video was accompanied by a comment from Cllr Boyes linking the ‘state’ of the tables with Travellers. That post attracted a number of comments which he liked.
[3/16]
Those liked comments included:
▪️ ‘scum should be f**k*ng shot oxygen thieves’ [edited]
▪️ ‘And they wonder why many people do not welcome them’.
[4/16]
Cllr Boyes accepted at the hearing that he did not have proof that Travellers caused the damage and that it was wrong for him to so implicate Travellers.
[5/16]
The press are now also covering Durham's decision to hold the hearing into the complaint against Cllr Boyes behind closed doors. See this item by @JHarrisonLDR, which includes reference to representations by @GypsyTravellers for a public hearing.https://t.co/C6M4KR65cW https://t.co/LuS8jQ2moi
— Dermot Feenan (@dermotfeenan) December 15, 2020
The grounds for the complaint are already set out by me: https://t.co/0MDqO6dyja. In summary: on 7 May 2020, Cllr Boyes posted on a Facebook site he shared with another councillor a video of scorch damage from barbeque trays and littering on and around a picnic table.
[2/16]
For those unfamiliar with the details of this complaint, I set out the basis of the complaint in the following 7 images:
— Dermot Feenan (@dermotfeenan) November 11, 2020
[8/14] pic.twitter.com/wrU18mBlMa
The table was in a picnic area in a nature reserve in the Easington constituency which Cllr Boyes represents. The video was accompanied by a comment from Cllr Boyes linking the ‘state’ of the tables with Travellers. That post attracted a number of comments which he liked.
[3/16]
Those liked comments included:
▪️ ‘scum should be f**k*ng shot oxygen thieves’ [edited]
▪️ ‘And they wonder why many people do not welcome them’.
[4/16]
Cllr Boyes accepted at the hearing that he did not have proof that Travellers caused the damage and that it was wrong for him to so implicate Travellers.
[5/16]


You May Also Like







Facebook originally a CIA program called "LifeLog".
LifeLog, via DARPA, terminated on Feb 4th, 2004.
Facebook was launched on Feb 4th, 2004.
Many of the LifeLog team became execs at FB.
Zuckerberg is a figurehead.
CIA allowed Cambridge to help Trump win
https://t.co/enzOXDCogV

Pentagon Kills LifeLog
LifeLog, via DARPA, terminated on Feb 4th, 2004.
Facebook was launched on Feb 4th, 2004.
Many of the LifeLog team became execs at FB.
Zuckerberg is a figurehead.
CIA allowed Cambridge to help Trump win
https://t.co/enzOXDCogV
Project: Lifelog
— Robert Horan (@Robby12692) December 13, 2018
Started by DARPA in 1999, the goal of Lifelog was to create a database on civilians without their knowledge, and track everything they do.
The project "ended" on Feb 4th, 2004.
Facebook began the exact same day.
The CIA funneled tens of millions into Facebook. pic.twitter.com/r7hwF0v9kh
Pentagon Kills LifeLog



Took me 5 years to get the best Chartink scanners for Stock Market, but you’ll get it in 5 mminutes here ⏰
Do Share the above tweet 👆
These are going to be very simple yet effective pure price action based scanners, no fancy indicators nothing - hope you liked it.
https://t.co/JU0MJIbpRV
52 Week High
One of the classic scanners very you will get strong stocks to Bet on.
https://t.co/V69th0jwBr
Hourly Breakout
This scanner will give you short term bet breakouts like hourly or 2Hr breakout
Volume shocker
Volume spurt in a stock with massive X times
Do Share the above tweet 👆
These are going to be very simple yet effective pure price action based scanners, no fancy indicators nothing - hope you liked it.
https://t.co/JU0MJIbpRV
52 Week High
One of the classic scanners very you will get strong stocks to Bet on.
https://t.co/V69th0jwBr
Hourly Breakout
This scanner will give you short term bet breakouts like hourly or 2Hr breakout
Volume shocker
Volume spurt in a stock with massive X times




