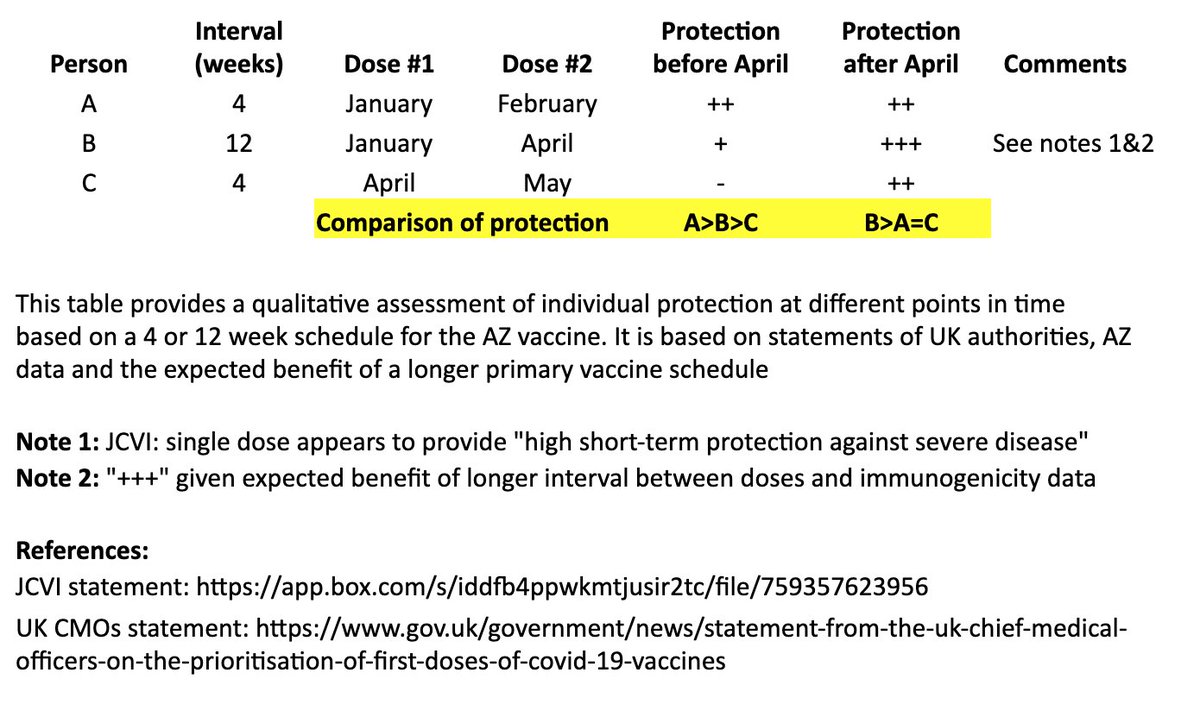
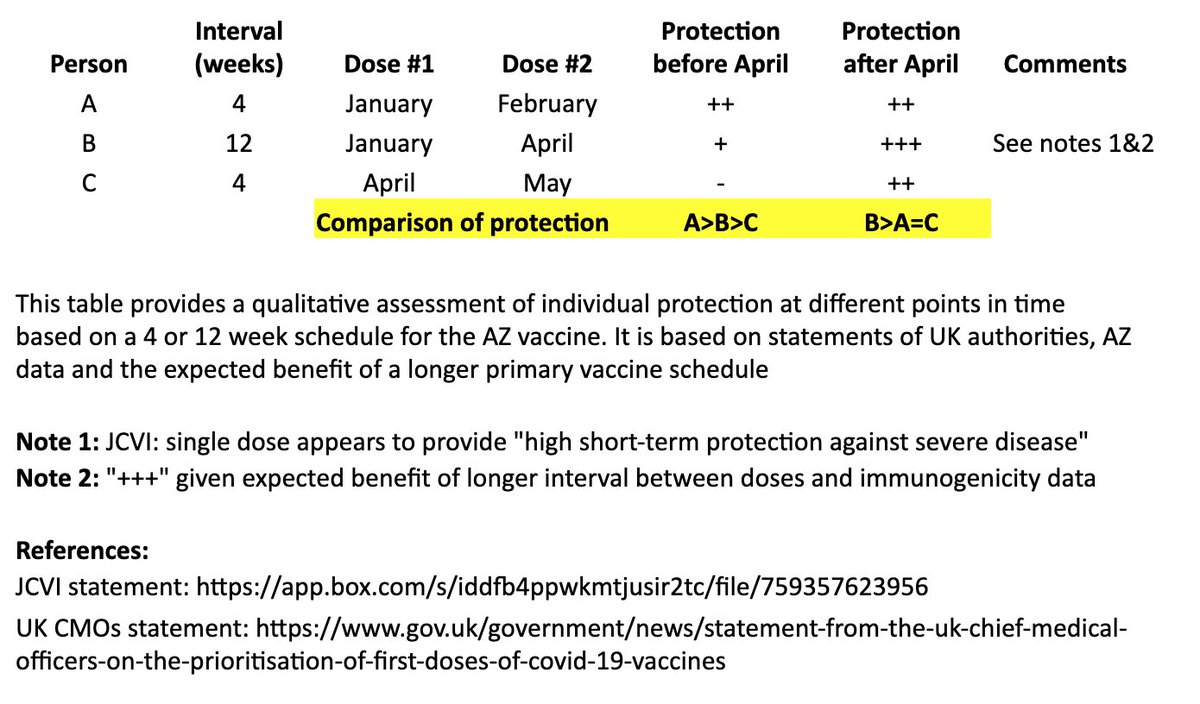
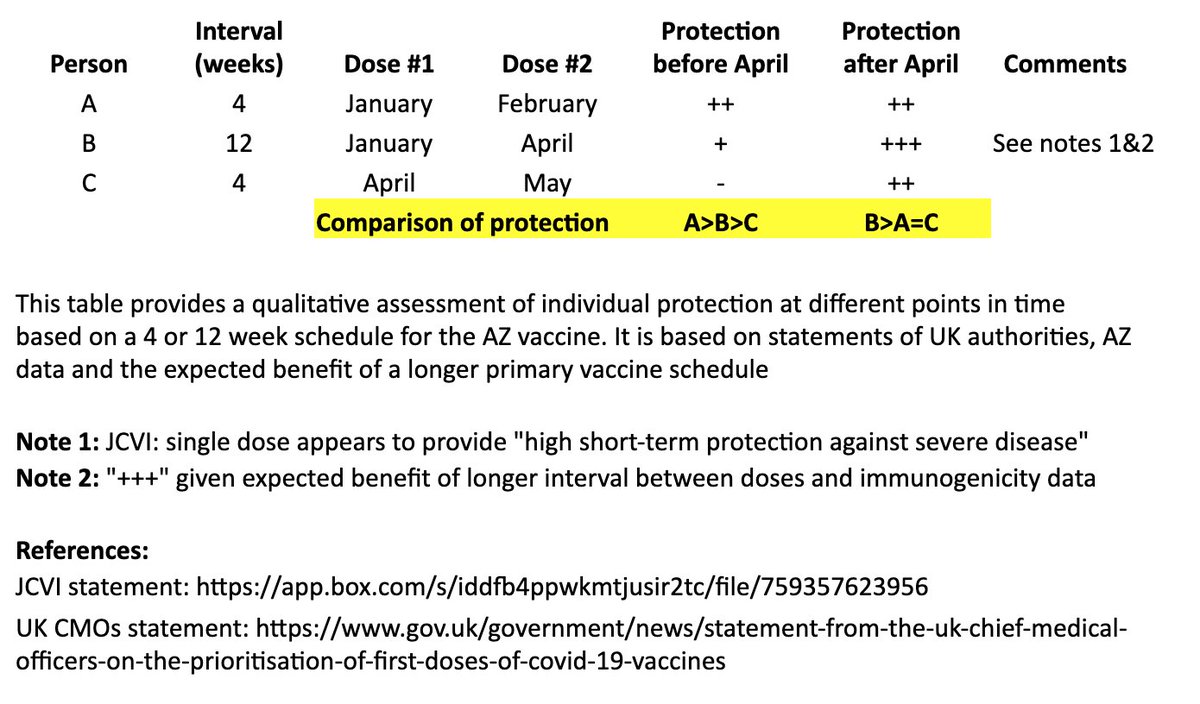
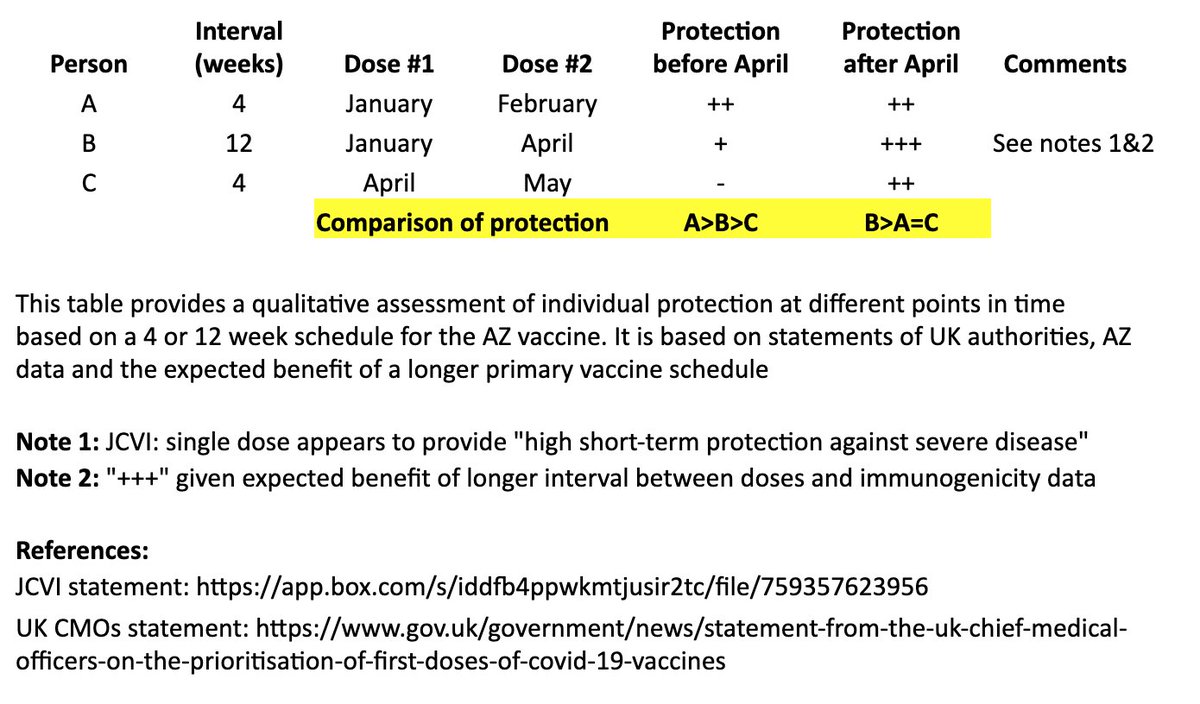
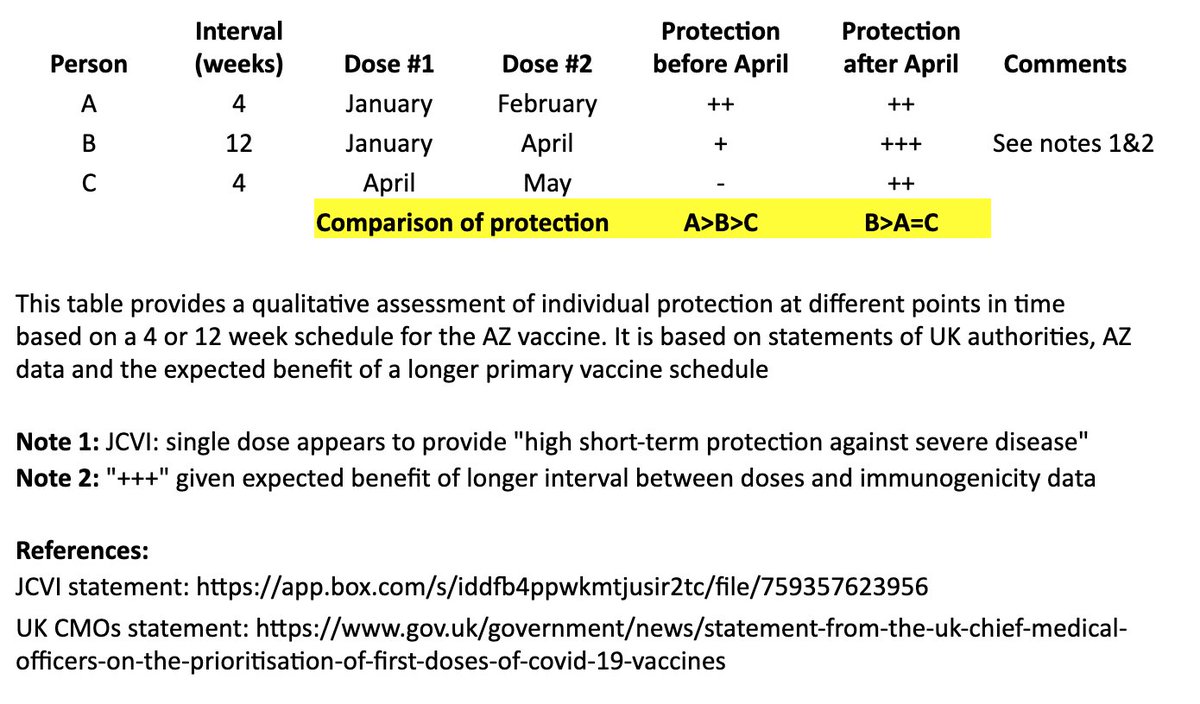
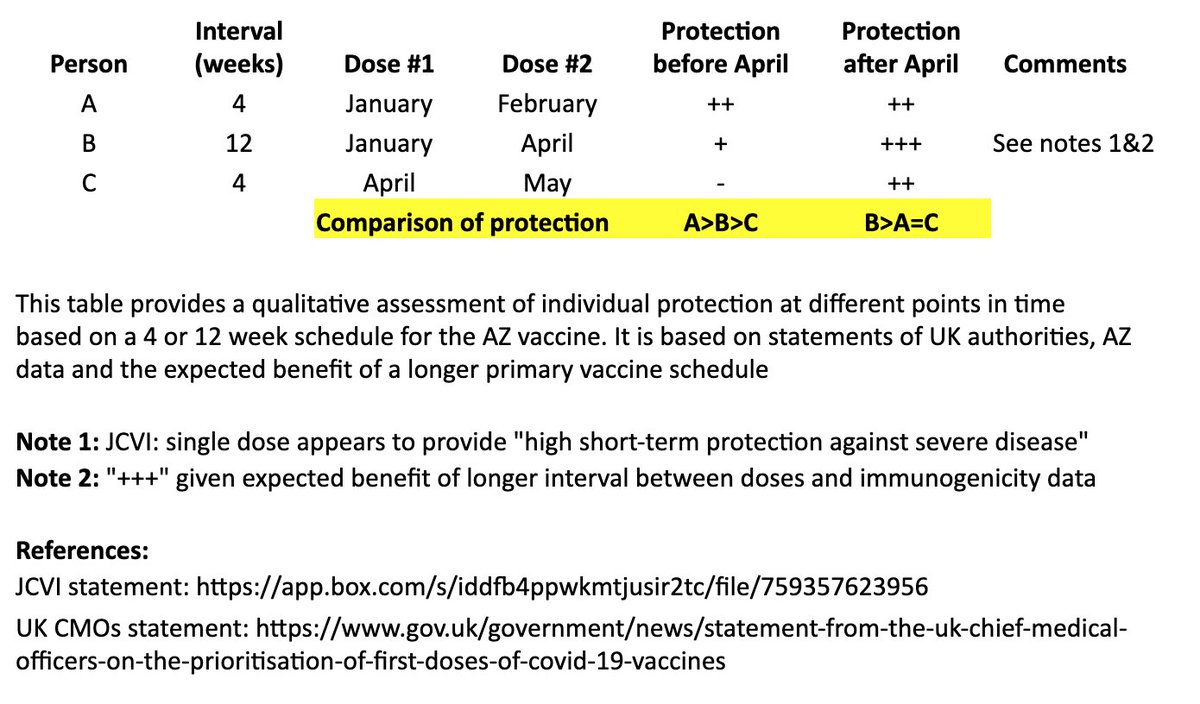
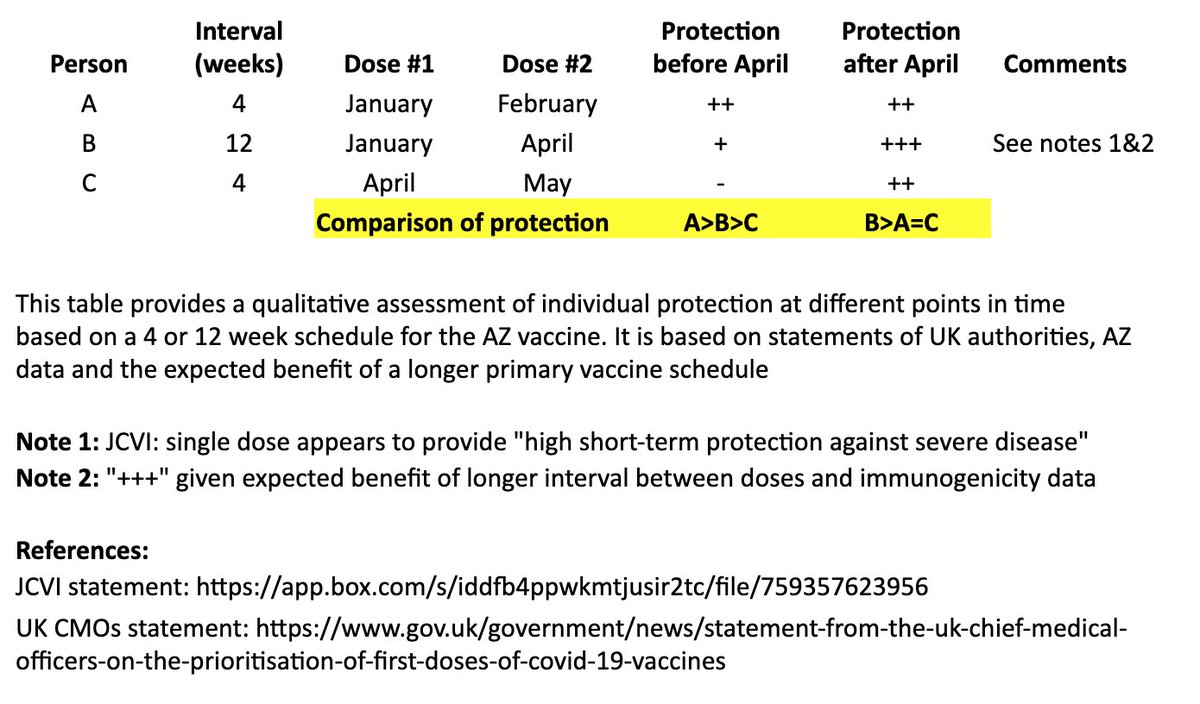
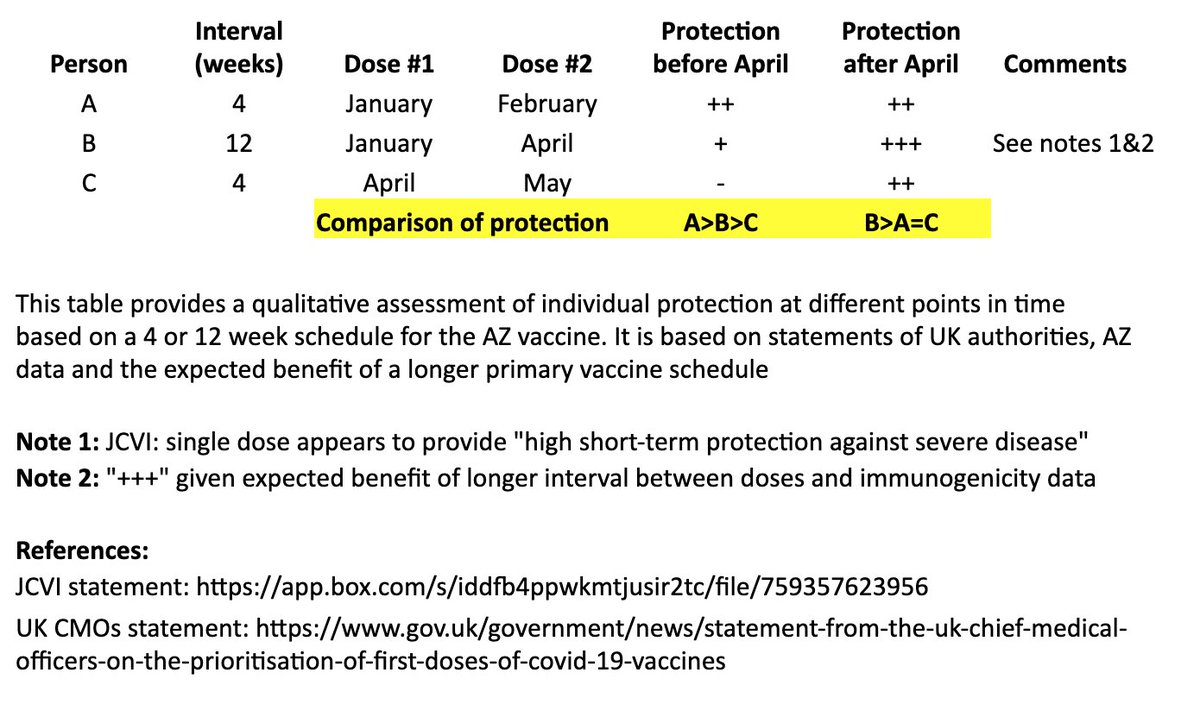
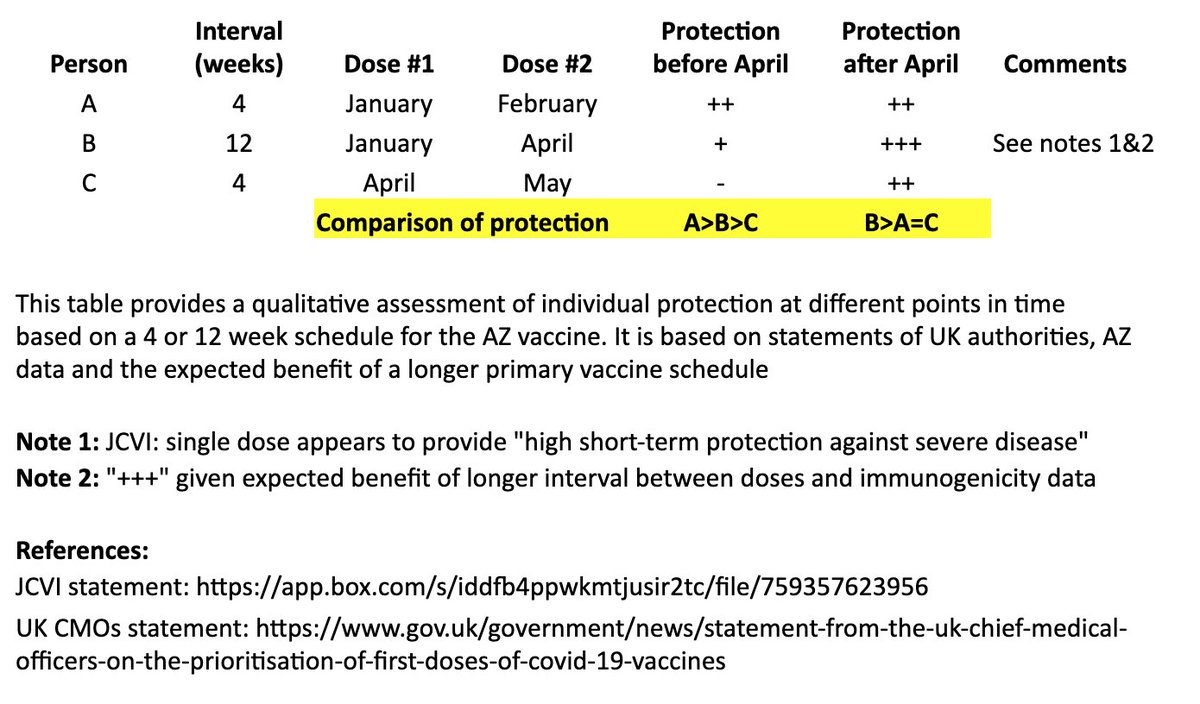
JCVI: https://t.co/6FQ25d6MFE
UK Chief Medical Officer (CMO) statement: https://t.co/RTpAIqgE1i
CMO letter to the profession: https://t.co/4WeexrVYWX
In @washingtonpost, @ashishkjha & I argue for the 2nd-shot-deferred strategy, partly by invoking the Mike Tyson principle. https://t.co/ZxrgVj3TJe We both came to this view because of the slow rollout & the new variant. But it's a tough call and reasonable people will disagree.
— Bob Wachter (@Bob_Wachter) January 3, 2021
This issue is, appropriately, contentious. As a vaccinologist - & citizen & relative of people in at-risk groups - I fully support the UK decision to increase dose intervals of both our Ox/AZ product and the Pfizer product. I'd happily receive either with a >8w gap. Here's why \U0001f9f5 https://t.co/PZaxgGJUj4
— Sandy Douglas (@sandyddouglas) January 1, 2021
THREAD
— Rajeev Venkayya MD (@rvenkayya) January 1, 2021
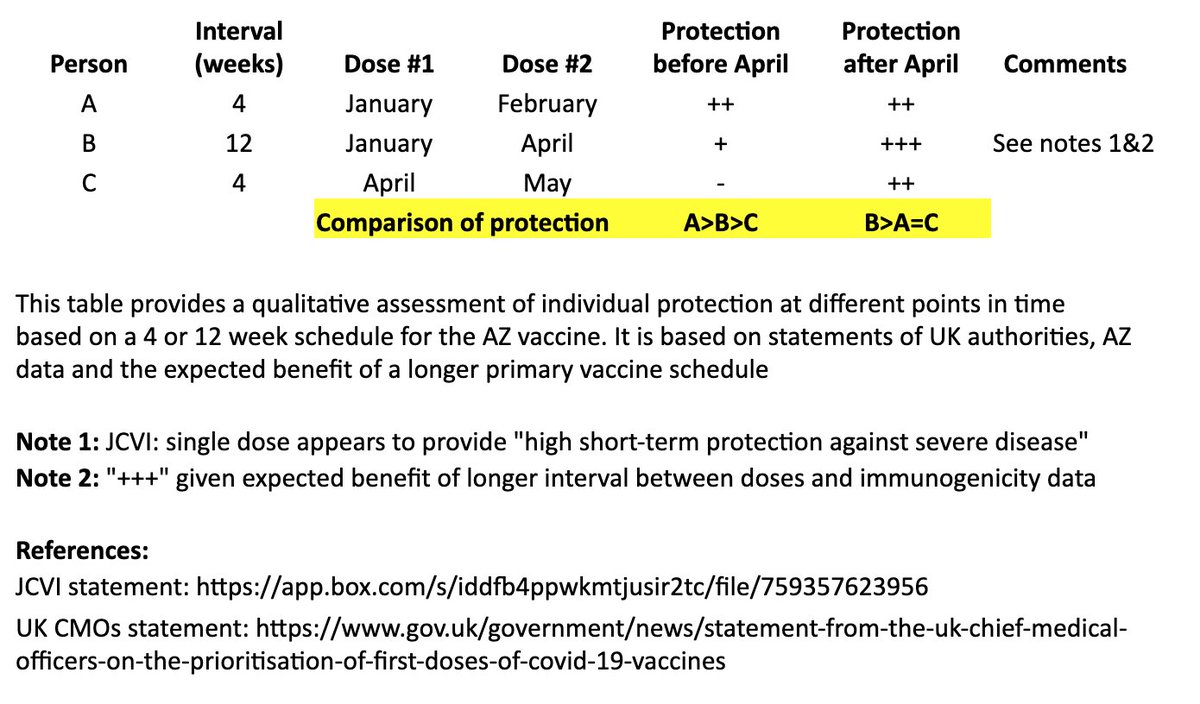
There\u2019s much debate around the UK's recommended use of the AZ vaccine with a two-dose schedule and flexible timing of second dose. Some thoughts on the AZ recommendation (not Pfizer) based on available data with refs to some excellent threads. 1/https://t.co/IFOC9M6vkq

Project: Lifelog
— Robert Horan (@Robby12692) December 13, 2018
Started by DARPA in 1999, the goal of Lifelog was to create a database on civilians without their knowledge, and track everything they do.
The project "ended" on Feb 4th, 2004.
Facebook began the exact same day.
The CIA funneled tens of millions into Facebook. pic.twitter.com/r7hwF0v9kh