
She was asked about “Post Exertional Malaise”... 2/n
I held back from commenting overnight to chew it over, but I am still saddened by comments during a presentation I attended yesterday by Prof @trishgreenhalgh & @CIHR_IMHA.
The topic was “LongCovid, Myalgic Encephalomyelitis & More”.
I quote from memory.
1/n
#MECFS #LongCovid
Have you registered for IMHA's next webinar on Long-COVID? Guest speaker Professor Trisha Greenhalgh.
— CIHR-IMHA Community (@CIHR_IMHA) January 12, 2021
When? Tomorrow: *Jan 13th.* 12pm ET
A few spots are left, but going fast!
Registration required: https://t.co/T4PbWNA35Y@KarimKhan_IMHA @CIHR_IRSC @trishgreenhalgh pic.twitter.com/xlWKi4QKF1
She was asked about “Post Exertional Malaise”... 2/n
@Trishgreenhalgh acknowledged the new @NiceComms advice for LongCovid was planned to complement... 3/n
Then it all went wrong.
@TrishGreenhalgh noted the changes to the @NiceComms guidance for ME/CFS, removing support for Graded Exercise Therapy / Cognitive Behavioural Therapy. She noted there is a big debate about this. 4/n
https://t.co/0enH8TFPoe
However Prof Greenhalgh then went off-piste.
5/n
6/n
Aside from ethical issues of naming patients, this is an n=1 case.
7/n
Furthermore, @TrishGreenhalgh failed to mention Prof Jonathan Edwards’ (not on twitter) Expert Testimony.
8/n
His testimony can be found here:
https://t.co/qLhsBJ4Bcu
9/n
I find this ill-befitting of an academic of her standing.
10/n
It puts her view in the field of politics not medicine.
That opens her to political-style criticism, which would be a shame.
11/n
We must play the ball, not the player.
12/n
Perhaps that is why, between 2015-2016 only £5m / year was spent on researching the condition.
Or aproximatly £0.35p per person, per year. Ouch.
https://t.co/TUPEiSCLZq
13/n
It really hurts.
And how ‘aggressive’ were these patients? Is this tweet aggressive? Will I be blocked and blamed?
14/n
I have a fatiguing gut condition and was mis-diagnosed with ME/CFS 4 years ago. I walked 6Km / day.
A specialist ‘undiagnosed’ me as I did not have PEM.
But in 2005, could I have been eligible for a GET study, and might have felt better after exercise.
15/n
She likes to go for walks, and exercises when she can. Had she taken up the offer to participate in a trial, she may have improved too.
16/n
I also experienced gas-lighting from the 20+ docs who told me it was all in my head. Thankfully I now have much better medical support, but many struggle.
17/n
The condition needs research, and that starts with belief, and develops with high-quality, objective science.
END/
I am actually a big supporter of Prof Greenhalgh’s work. Masks are good. So is good patient care.
I have no malicious intent, but it is right to challenge bad pronouncements on this issue.

If you think I have got it wrong, please let me know.
Please challenge misinformation about on ME/CFS, but accept that even great people make mistakes. Forgive.
More from Education



Department List of UCAS-China PROFESSORs for ANSO, CSC and UCAS (fully or partial) Scholarship Acceptance
1) UCAS School of physical sciences Professor
https://t.co/9X8OheIvRw
2) UCAS School of mathematical sciences Professor
3) UCAS School of nuclear sciences and technology
https://t.co/nQH8JnewcJ
4) UCAS School of astronomy and space sciences
https://t.co/7Ikc6CuKHZ
5) UCAS School of engineering
6) Geotechnical Engineering Teaching and Research Office
https://t.co/jBCJW7UKlQ
7) Multi-scale Mechanics Teaching and Research Section
https://t.co/eqfQnX1LEQ
😎 Microgravity Science Teaching and Research
9) High temperature gas dynamics teaching and research section
https://t.co/tVIdKgTPl3
10) Department of Biomechanics and Medical Engineering
https://t.co/ubW4xhZY2R
11) Ocean Engineering Teaching and Research
12) Department of Dynamics and Advanced Manufacturing
https://t.co/42BKXEugGv
13) Refrigeration and Cryogenic Engineering Teaching and Research Office
https://t.co/pZdUXFTvw3
14) Power Machinery and Engineering Teaching and Research
1) UCAS School of physical sciences Professor
https://t.co/9X8OheIvRw
2) UCAS School of mathematical sciences Professor
3) UCAS School of nuclear sciences and technology
https://t.co/nQH8JnewcJ
4) UCAS School of astronomy and space sciences
https://t.co/7Ikc6CuKHZ
5) UCAS School of engineering
6) Geotechnical Engineering Teaching and Research Office
https://t.co/jBCJW7UKlQ
7) Multi-scale Mechanics Teaching and Research Section
https://t.co/eqfQnX1LEQ
😎 Microgravity Science Teaching and Research
9) High temperature gas dynamics teaching and research section
https://t.co/tVIdKgTPl3
10) Department of Biomechanics and Medical Engineering
https://t.co/ubW4xhZY2R
11) Ocean Engineering Teaching and Research
12) Department of Dynamics and Advanced Manufacturing
https://t.co/42BKXEugGv
13) Refrigeration and Cryogenic Engineering Teaching and Research Office
https://t.co/pZdUXFTvw3
14) Power Machinery and Engineering Teaching and Research

Admission and Scholarship in Germany (Part A)
As promised, let's start the year by discussing Germany.
Tag your friends, take fruit juice and unwind this thread🧵:
In Part A, I will discuss what you need to know about Admission and Scholarship in Germany, In Part B, I will show you how to practically apply and get funding.
Read the following general facts about Germany:
1. About 80-90% of the Universities are tuition-free.
However, in some states, you may be asked to pay about 1000-3000 Euros/semester, which covers student union fees and travel tickets around the state for a semester.
2. Most Msc students don't search for scholarships. Instead, they look for a block account of about 10, 000
Euros.
Read: https://t.co/sg9sZomuxA.
3. From the block account, the Govt pays you about 850 Euros monthly for Living expenses.
Check:
4. If you can find a way to get the block account, you have the chance of recouping your money back and much more because student job is around 1000 Euros/month, and it's about 20-40hrs /week.
Read:
As promised, let's start the year by discussing Germany.
Tag your friends, take fruit juice and unwind this thread🧵:
In Part A, I will discuss what you need to know about Admission and Scholarship in Germany, In Part B, I will show you how to practically apply and get funding.
Read the following general facts about Germany:
1. About 80-90% of the Universities are tuition-free.
However, in some states, you may be asked to pay about 1000-3000 Euros/semester, which covers student union fees and travel tickets around the state for a semester.
2. Most Msc students don't search for scholarships. Instead, they look for a block account of about 10, 000
Euros.
Read: https://t.co/sg9sZomuxA.
3. From the block account, the Govt pays you about 850 Euros monthly for Living expenses.
Check:
4. If you can find a way to get the block account, you have the chance of recouping your money back and much more because student job is around 1000 Euros/month, and it's about 20-40hrs /week.
Read:


You asked. So here are my thoughts on how osteopathic medical students should respond to the NBOME.
(thread)
Look, even before the Step 2 CS cancellation, my DMs and email were flooded with messages from osteopathic medical students who are fed up with the NBOME.
There is *real* anger toward this organization. Honestly, more than I even heard about from MD students and the NBME.
The question is, will that sentiment translate into action?
Amorphous anger on social media is easy to ignore. But if that anger gets channeled into organized efforts to facilitate change, then improvements are possible.
This much should be clear: begging the NBOME to reconsider their Level 2-PE exam is a waste of your time.
Best case scenario, you’ll get another “town hall” meeting, a handful of platitudes, and some thoughtful beard stroking before being told that they’re keeping the exam.
Instead of complaining to the NBOME, here are a few things that are more likely to bring about real change.
(thread)
I think most of us are over here waiting to see what @jbcarmody has to say about the latest NBOME email pic.twitter.com/bVWkS23V7z
— Jake Berg (@jberg521) January 28, 2021
Look, even before the Step 2 CS cancellation, my DMs and email were flooded with messages from osteopathic medical students who are fed up with the NBOME.
There is *real* anger toward this organization. Honestly, more than I even heard about from MD students and the NBME.
The question is, will that sentiment translate into action?
Amorphous anger on social media is easy to ignore. But if that anger gets channeled into organized efforts to facilitate change, then improvements are possible.
This much should be clear: begging the NBOME to reconsider their Level 2-PE exam is a waste of your time.
Best case scenario, you’ll get another “town hall” meeting, a handful of platitudes, and some thoughtful beard stroking before being told that they’re keeping the exam.
Instead of complaining to the NBOME, here are a few things that are more likely to bring about real change.
You May Also Like















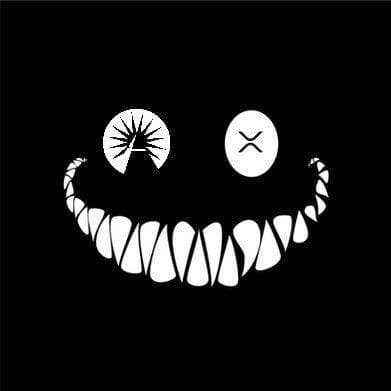
The Eye of Horus. 1/*
I believe that @ripple_crippler and @looP_rM311_7211 are the same person. I know, nobody believes that. 2/*
Today I want to prove that Mr Pool smile faces mean XRP and price increase. In Ripple_Crippler, previous to Mr Pool existence, smile faces were frequent. They were very similar to the ones Mr Pool posts. The eyes also were usually a couple of "x", in fact, XRP logo. 3/*

The smile XRP-eyed face also appears related to the Moon. XRP going to the Moon. 4/*

And smile XRP-eyed faces also appear related to Egypt. In particular, to the Eye of Horus. https://t.co/i4rRzuQ0gZ 5/*
I believe that @ripple_crippler and @looP_rM311_7211 are the same person. I know, nobody believes that. 2/*
Today I want to prove that Mr Pool smile faces mean XRP and price increase. In Ripple_Crippler, previous to Mr Pool existence, smile faces were frequent. They were very similar to the ones Mr Pool posts. The eyes also were usually a couple of "x", in fact, XRP logo. 3/*
The smile XRP-eyed face also appears related to the Moon. XRP going to the Moon. 4/*
And smile XRP-eyed faces also appear related to Egypt. In particular, to the Eye of Horus. https://t.co/i4rRzuQ0gZ 5/*