
Also, scientists stand apart from their subject matter--as distantly as possible. Physicians, on the contrary, are in "a relationship" with patients. 2/
Sorry, Dr. Jha, but you shouldn't confuse medical care with the scientific enterprise. Although the 2 are commonly conflated, they are really distinct. 1/
The hearings are meant as a questioning of the scientific process
— Ashish K. Jha, MD, MPH (@ashishkjha) December 7, 2020
To sew doubt on what we know and how we know it
So a group of us organized a response, which we just posted on our website
It isn't pro or anti hydroxy
Its about the scientific method and why it matters
2/3
Also, scientists stand apart from their subject matter--as distantly as possible. Physicians, on the contrary, are in "a relationship" with patients. 2/
First, scientific knowledge is often limited or provisional, especially with a new disease.
Second, for every patient there are myriad circumstances that influence a medical decision. /3
Fourth--and most pertinent here--one cannot narrowly limit the scientific knowledge to only RCTs as you do in your statement. /4
I won't rehash all the arguments here (and there are many!) but I'm sure you're familiar with this piece by Dr. Frieden from only a couple of years ago https://t.co/f7jHvDujUZ /5
My point is that your attacks miss the point: Medical standards cannot be reduced to scientific ones. /12
If you have an interest in the historical background for this, here are a couple of the pieces that I wrote on this topic a few years ago: /14
https://t.co/q5ECfaN47b
More from Science


JUST ONE PERSON—UK 🇬🇧 scientists think one immunocompromised person who cleared virus slowly & only partially wiped out an infection, leaving behind genetically-hardier viruses that rebound & learn how to survive better. That’s likely how #B117 started. 🧵 https://t.co/bMMjM8Hiuz
2) The leading hypothesis is that the new variant evolved within just one person, chronically infected with the virus for so long it was able to evolve into a new, more infectious form.
same thing happened in Boston in another immunocompromised person that was sick for 155 days.
3) What happened in Boston with one 45 year old man who was highly infectious for 155 days straight before he died... is exactly what scientists think happened in Kent, England that gave rise to #B117.
4) Doctors were shocked to find virus has evolved many different forms inside of this one immunocompromised man. 20 new mutations in one virus, akin to the #B117. This is possibly how #B1351 in South Africa 🇿🇦 and #P1 in Brazil 🇧🇷 also evolved.
5) “On its own, the appearance of a new variant in genomic databases doesn’t tell us much. “That’s just one genome amongst thousands every week. It wouldn’t necessarily stick out,” says Oliver Pybus, a professor of evolution and infectious disease at Oxford.
2) The leading hypothesis is that the new variant evolved within just one person, chronically infected with the virus for so long it was able to evolve into a new, more infectious form.
same thing happened in Boston in another immunocompromised person that was sick for 155 days.
3) What happened in Boston with one 45 year old man who was highly infectious for 155 days straight before he died... is exactly what scientists think happened in Kent, England that gave rise to #B117.
Immunocompromised 45 year old suffered from #COVID19 for 155 days before he died. The virus was changing very quickly inside the man's body\u2014it acquired a big cluster of >20 mutations\u2014resembled the same ones seen in #B117 & #B1351. (NPR audio Part 1 of 2)\U0001f9f5https://t.co/7kWiBZ1xGk pic.twitter.com/ZJ7AExB78Y
— Eric Feigl-Ding (@DrEricDing) February 8, 2021
4) Doctors were shocked to find virus has evolved many different forms inside of this one immunocompromised man. 20 new mutations in one virus, akin to the #B117. This is possibly how #B1351 in South Africa 🇿🇦 and #P1 in Brazil 🇧🇷 also evolved.
2) NPR report audio part 2 of 2:
— Eric Feigl-Ding (@DrEricDing) February 8, 2021
Dr. Li couldn't believe what they found. "I was shocked," he says. "When I saw the virus sequences, I knew that we were dealing with something completely different and potentially very important." pic.twitter.com/HT3Yt6djFd
5) “On its own, the appearance of a new variant in genomic databases doesn’t tell us much. “That’s just one genome amongst thousands every week. It wouldn’t necessarily stick out,” says Oliver Pybus, a professor of evolution and infectious disease at Oxford.




1/ Automobiles and Intake Fraction. Since cars are back in the news I thought I would retweet this model result I offered in early April 2020. I focused only on 1 micron particles & accounted for windows completely closed & cracked slightly open.
2/ Related air exchange rates were based on experimental results in literature for mid-sized sedans. Particle deposition to indoor surfaces were accounted for, as the surface to volume ratio in a 3 m3 cab is large. An important outcome was the intake fraction (IF)
3/ Here, IF is the number of particles (or virions in collective particles) inhaled by a receptor DIVIDED BY the number or particles (or virions in collective particles) emitted by an infector.
4/ Integrated over the two hour drive (in this example) the IF for all windows closed & a receptor at rest is 0.08 (8% of what comes out of the infectors respiratory system ends up in the respiratory system of the receptor). 8%! That is a very high intake factor.
5/ With additional ventilation from cracking a window open drops the IF to 0.012 (1.2%) still relatively high. Can get lower by opening more windows.
Simulation: Riding in car for 120 min w/ infected passenger who seems fine other than a cough every few mins. (1) a lot of SARS-CoV-2 virus (in fine aerosol particles) accumulation in car cabin w/ windows closed; (2) cracking window open slightly = dramatic reduction. #COVID19 pic.twitter.com/bCmrmnLUPG
— Dr. Richard Corsi (@CorsIAQ) April 4, 2020
2/ Related air exchange rates were based on experimental results in literature for mid-sized sedans. Particle deposition to indoor surfaces were accounted for, as the surface to volume ratio in a 3 m3 cab is large. An important outcome was the intake fraction (IF)
3/ Here, IF is the number of particles (or virions in collective particles) inhaled by a receptor DIVIDED BY the number or particles (or virions in collective particles) emitted by an infector.
4/ Integrated over the two hour drive (in this example) the IF for all windows closed & a receptor at rest is 0.08 (8% of what comes out of the infectors respiratory system ends up in the respiratory system of the receptor). 8%! That is a very high intake factor.
5/ With additional ventilation from cracking a window open drops the IF to 0.012 (1.2%) still relatively high. Can get lower by opening more windows.
You May Also Like





#sculpture #story -
Chandesha-Anugraha Murti - One of the Sculpture in Brihadeshwara Temple at Gangaikonda Cholapuram - built by Raja Rajendra Chola I
This Sculpture depicts Bhagwan Shiva along with Devi Paravathi blessing Chandeshwara - one of the 63 Nayanmars.
#Thread

Chandeshwara/Chandikeshwara is regarded as custodian of Shiva Temple's wealth&most of Shiva temples in South India has separate sannathi for him.
His bhakti for Bhagwan Shiva elevated him as one of foremost among Nayanmars.
He gave importance to Shiva Pooja&protection of cows.

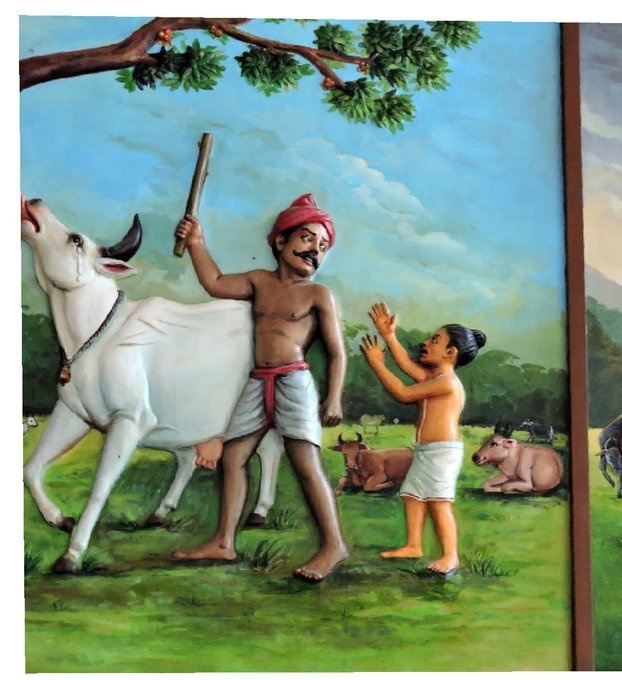
There are series of paintings, illustrating the #story of Chandikeshwar in the premises of
Sri Sathiyagireeswarar #Temple at Seinganur,near Kumbakonam,TN
Chandikeshwara's birth name
is Vichara sarman.He was born in the village of Senganur on the banks of River Manni.

His Parent names were Yajnathatan and Pavithrai.
Vichara Sarman was a gifted child and he learnt Vedas and Agamas at a very young age.
He was very devout and would always think about Bhagwan Shiva.
One day he saw a cowherd man brutally assaulting a cow,Vichara Sarman could not tolerate this. He spoke to cowherd: ‘Do you not know that the cow is worshipful & divine? All gods & Devas reside in https://t.co/ElLcI5ppsK it is our duty to protect cows &we should not to harm them.
Chandesha-Anugraha Murti - One of the Sculpture in Brihadeshwara Temple at Gangaikonda Cholapuram - built by Raja Rajendra Chola I
This Sculpture depicts Bhagwan Shiva along with Devi Paravathi blessing Chandeshwara - one of the 63 Nayanmars.
#Thread
Chandeshwara/Chandikeshwara is regarded as custodian of Shiva Temple's wealth&most of Shiva temples in South India has separate sannathi for him.
His bhakti for Bhagwan Shiva elevated him as one of foremost among Nayanmars.
He gave importance to Shiva Pooja&protection of cows.
There are series of paintings, illustrating the #story of Chandikeshwar in the premises of
Sri Sathiyagireeswarar #Temple at Seinganur,near Kumbakonam,TN
Chandikeshwara's birth name
is Vichara sarman.He was born in the village of Senganur on the banks of River Manni.
His Parent names were Yajnathatan and Pavithrai.
Vichara Sarman was a gifted child and he learnt Vedas and Agamas at a very young age.
He was very devout and would always think about Bhagwan Shiva.
One day he saw a cowherd man brutally assaulting a cow,Vichara Sarman could not tolerate this. He spoke to cowherd: ‘Do you not know that the cow is worshipful & divine? All gods & Devas reside in https://t.co/ElLcI5ppsK it is our duty to protect cows &we should not to harm them.





