It's Monday AM post-@ASCO #GU21 & clinic starts in a couple of hours! Lots to process - I'll try to tackle optimal 1L tx for #kidneycancer. I'll make a case for cabo/nivo, leaning on the beautiful (& timely) tables below from @lalaniMD, @SoaresAndrey & @brian_rini (1/15)
What about IO/IO? We have long f/u w #CM214 data w nivo/ipi, no doubt (@AlbigesL et al in @myESMO Open). And treatment-free interval discussed by McDermott @BIDMChealth is no doubt impt. But we've known data not as impressive for favorable risk (2/15)
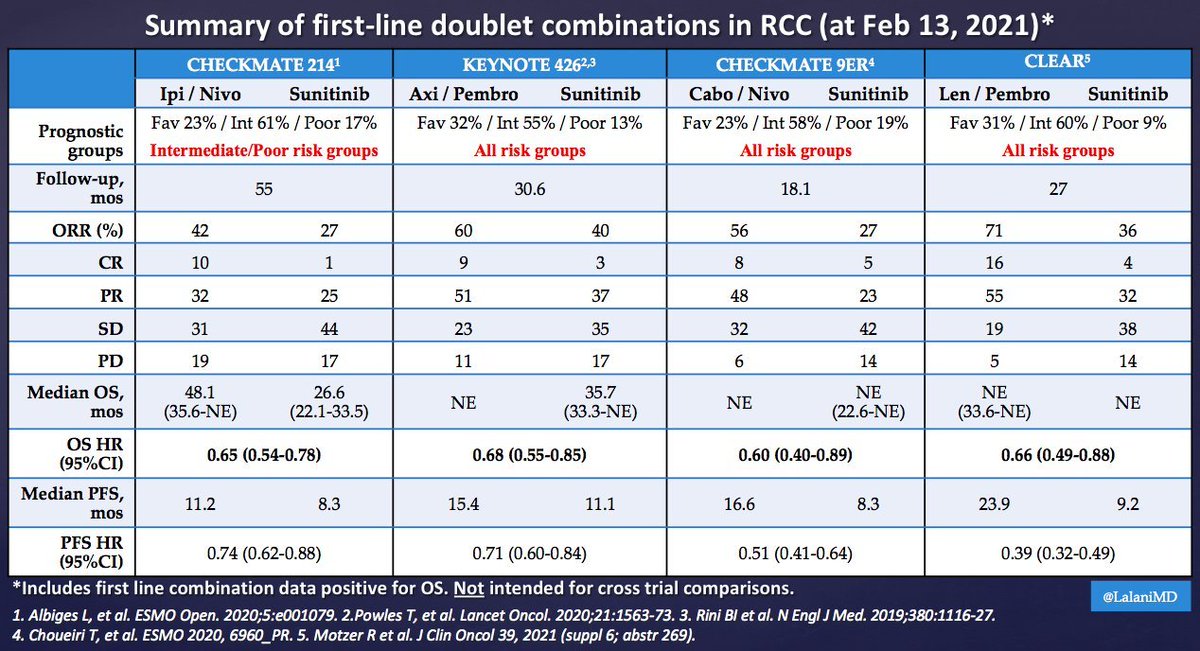
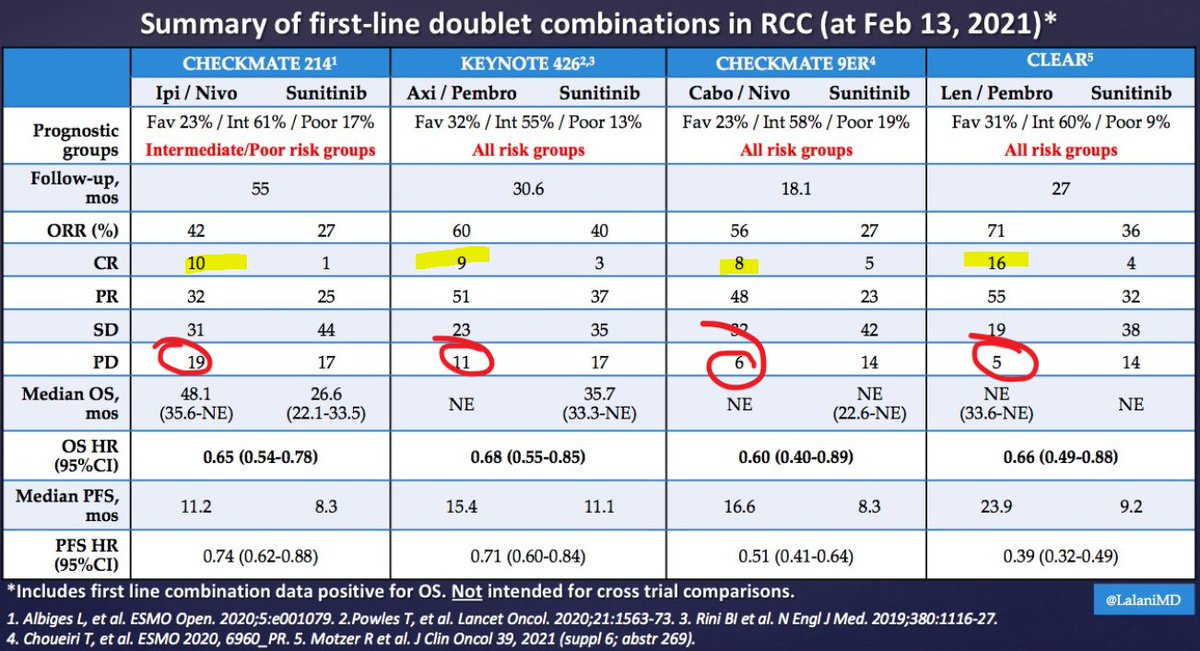
And furthermore, as @ERPlimackMD points out in another tweet, impt to look at primary PD rates (seen in @lalaniMD's table) - nivo/ipi at 19%!!! CR rate used to be something we highlighted w nivo/ipi, but now comparable across studies (3/15)
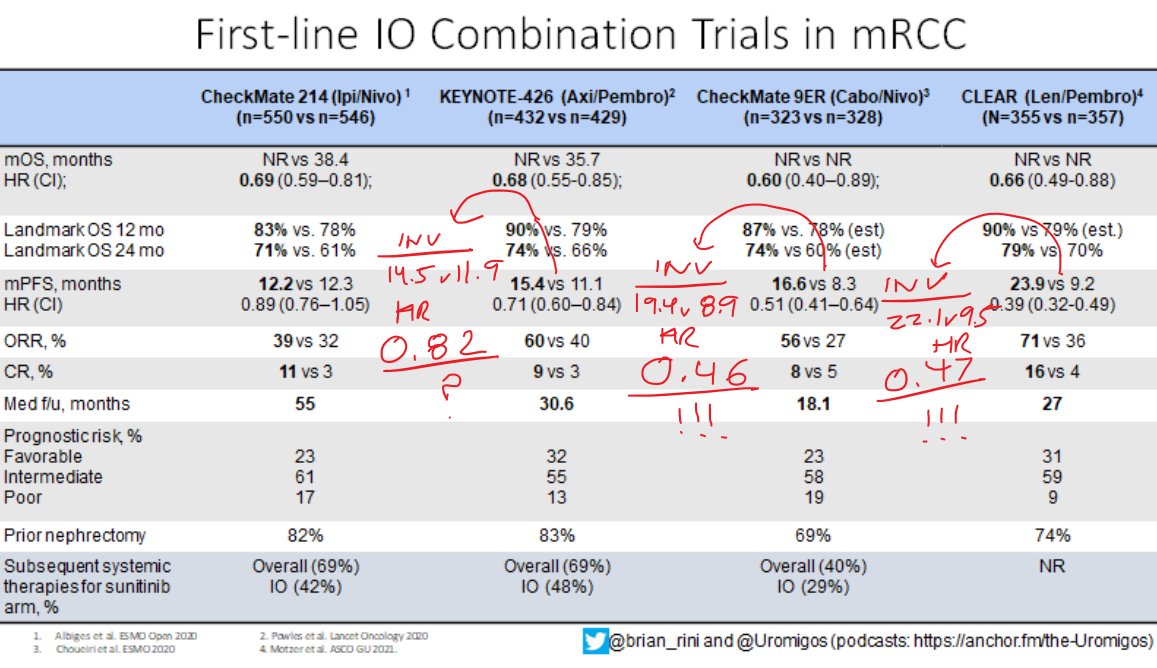
Okay now to the really tough stuff - comparing TKI/IO regimens. Something interesting I will add to @brian_rini @uromigos table above is the HR for PFS by INVESTIGATOR review. If the diff in HR for PFS by IND review caught your eye, this is even more striking (4/15)
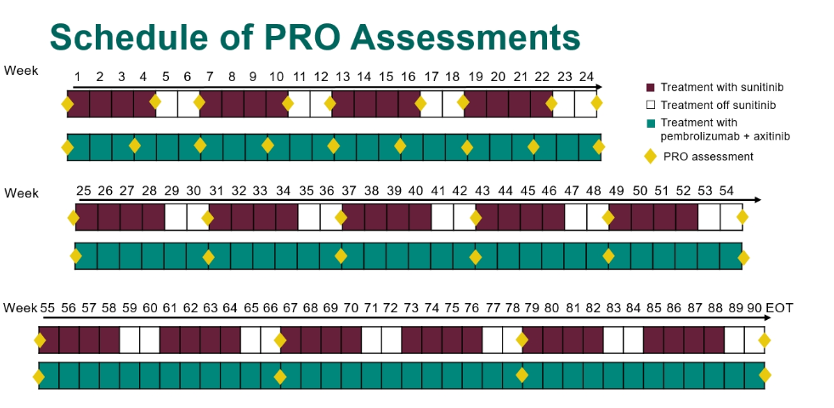
I think INV-assessed PFS is impt, but if you're a skeptic, forget that argument. Turn instead to #QOL with axi/pembro. Kudos to @brian_rini @tompowles1 @ERPlimackMD et al for advocating for QOL in KN-426. @crisbergerot et al have taughts us the importance of these metrics. (5/15)