
26/42 Are there any national datasets that accurately capture what is going on? The brilliant @jburnmurdoch has highlighted number of admissions into ICU. The message from his animated chart (click on link) couldn’t be clearer – this winter is v unusual: https://t.co/76ZvHU2pmV.
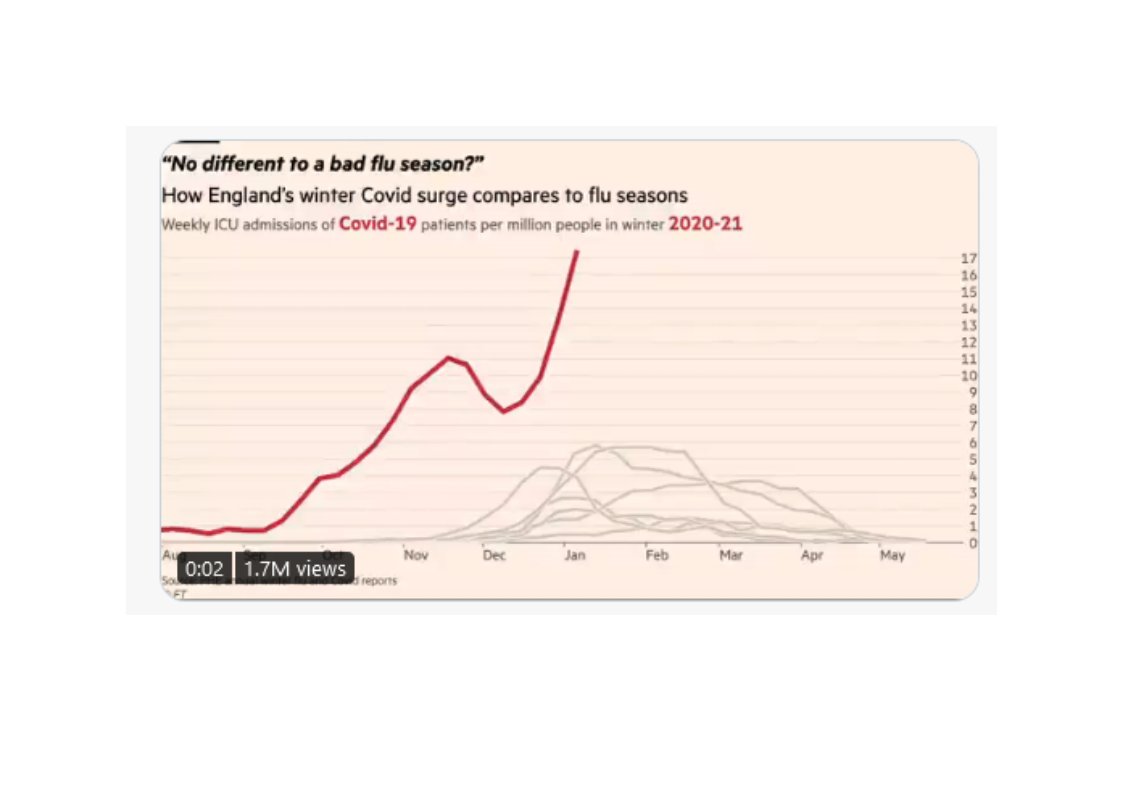
NEW: a common response to reports of hospitals struggling this winter is "it\u2019s no different to a bad flu season!"
— John Burn-Murdoch (@jburnmurdoch) January 7, 2021
I\u2019ve tracked down historical data on flu ICU admissions, including winter 2017-18, a record high.
Here\u2019s how England\u2019s Covid winter compares to a bad flu season \U0001f4f9 pic.twitter.com/tsExrDZM31
Here's a detailed thread explaining how the weekly ONS data should be interpreted when monitoring all cause mortality and excess deaths. It seems very common for people to misinterpret the data relating to excess deaths so I will do my best to clarify in a series of tweets. 1/10 pic.twitter.com/r2TUH7I4wE
— Michael George (@Mike_aka_Logiqx) January 9, 2021
To believe the hypothesis posed by the sceptics you also have to believe this. Either those charged with monitoring the nation\u2019s health \u2013 the CMO, CSA, their colleagues in the regions, Ministers, officials \u2013 are unaware of the data flaws Julia and her allies have identified...
— (((Dan Hodges))) (@DPJHodges) January 8, 2021
More from Health

1/16
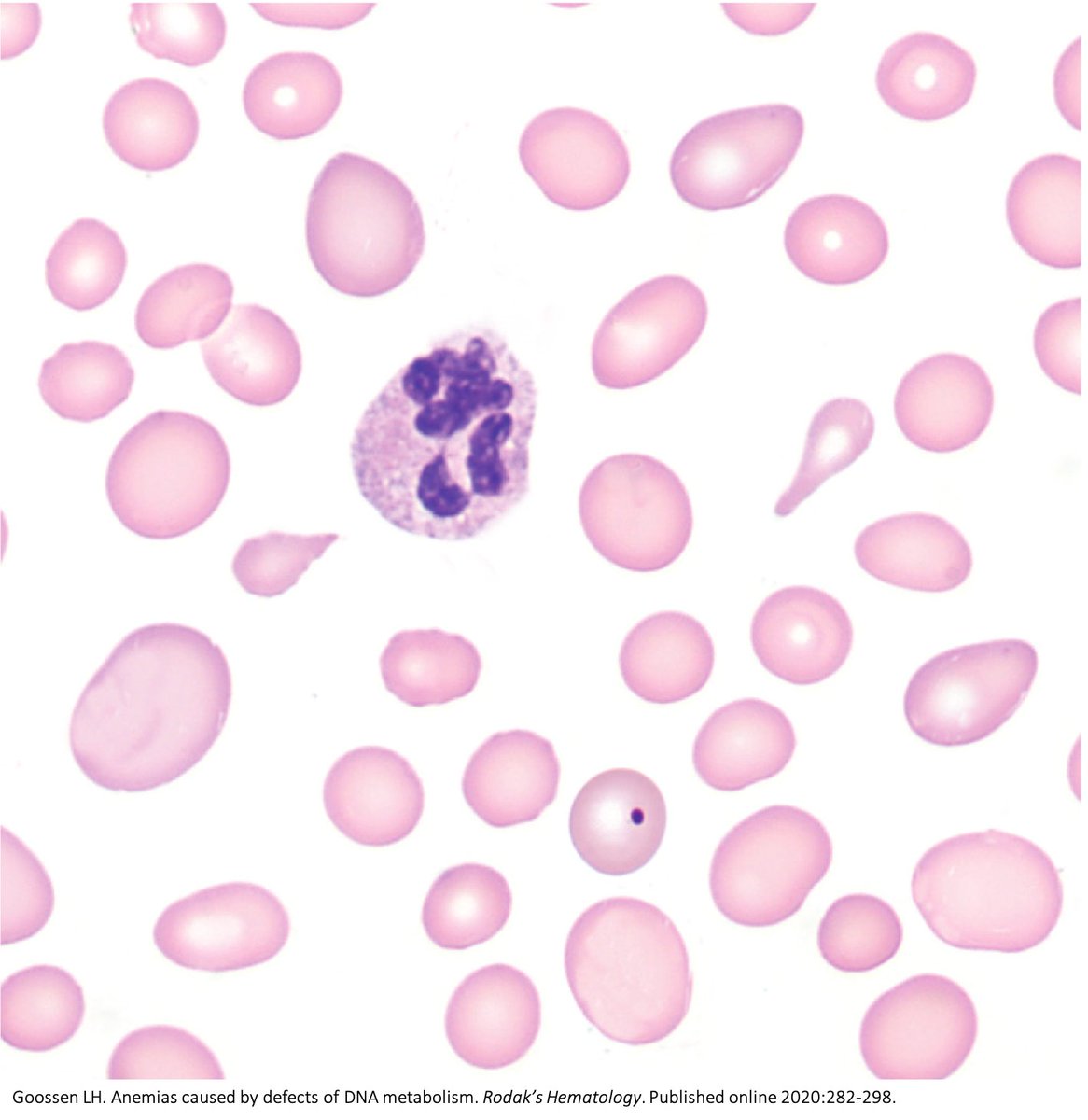
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
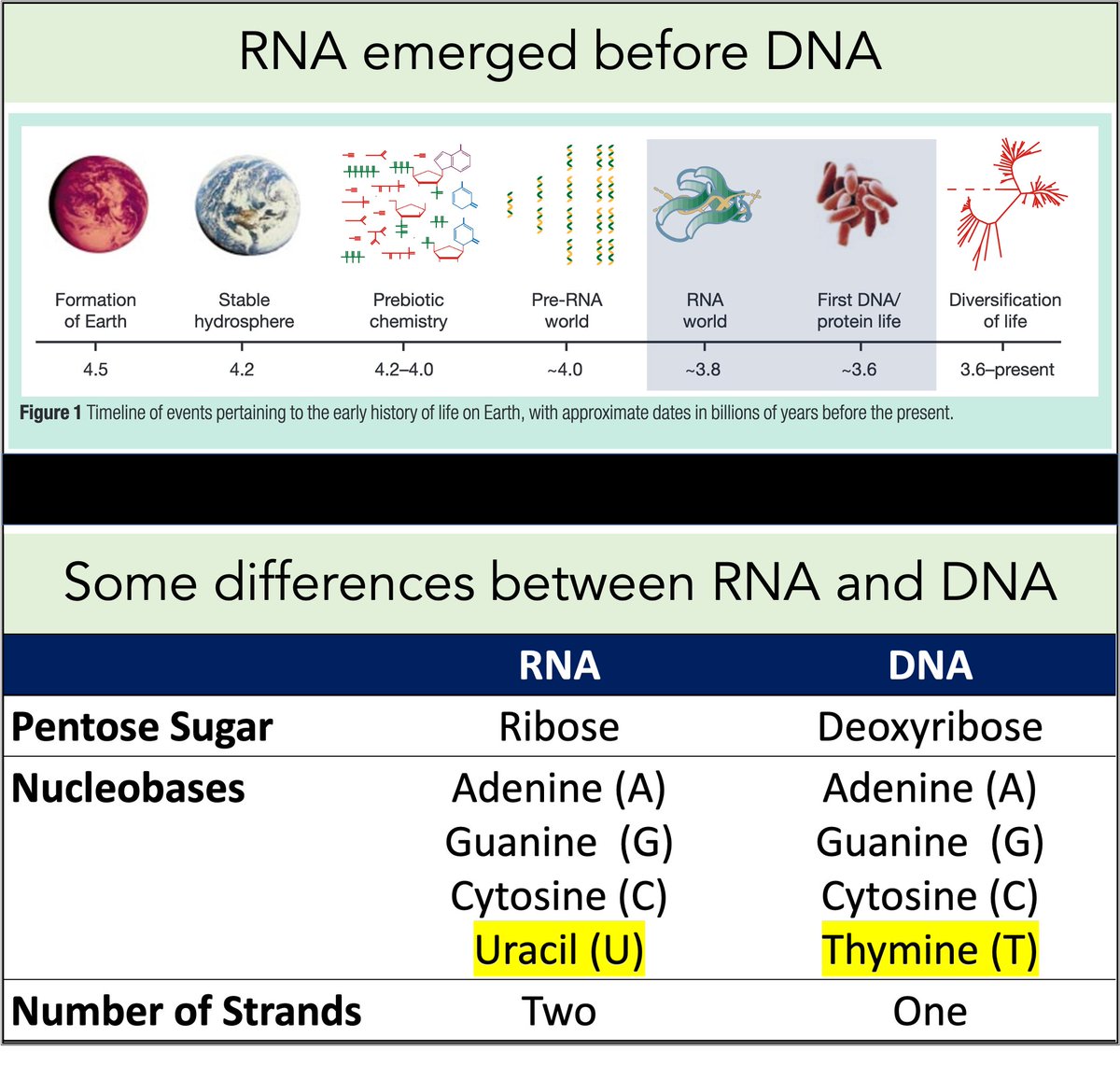
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
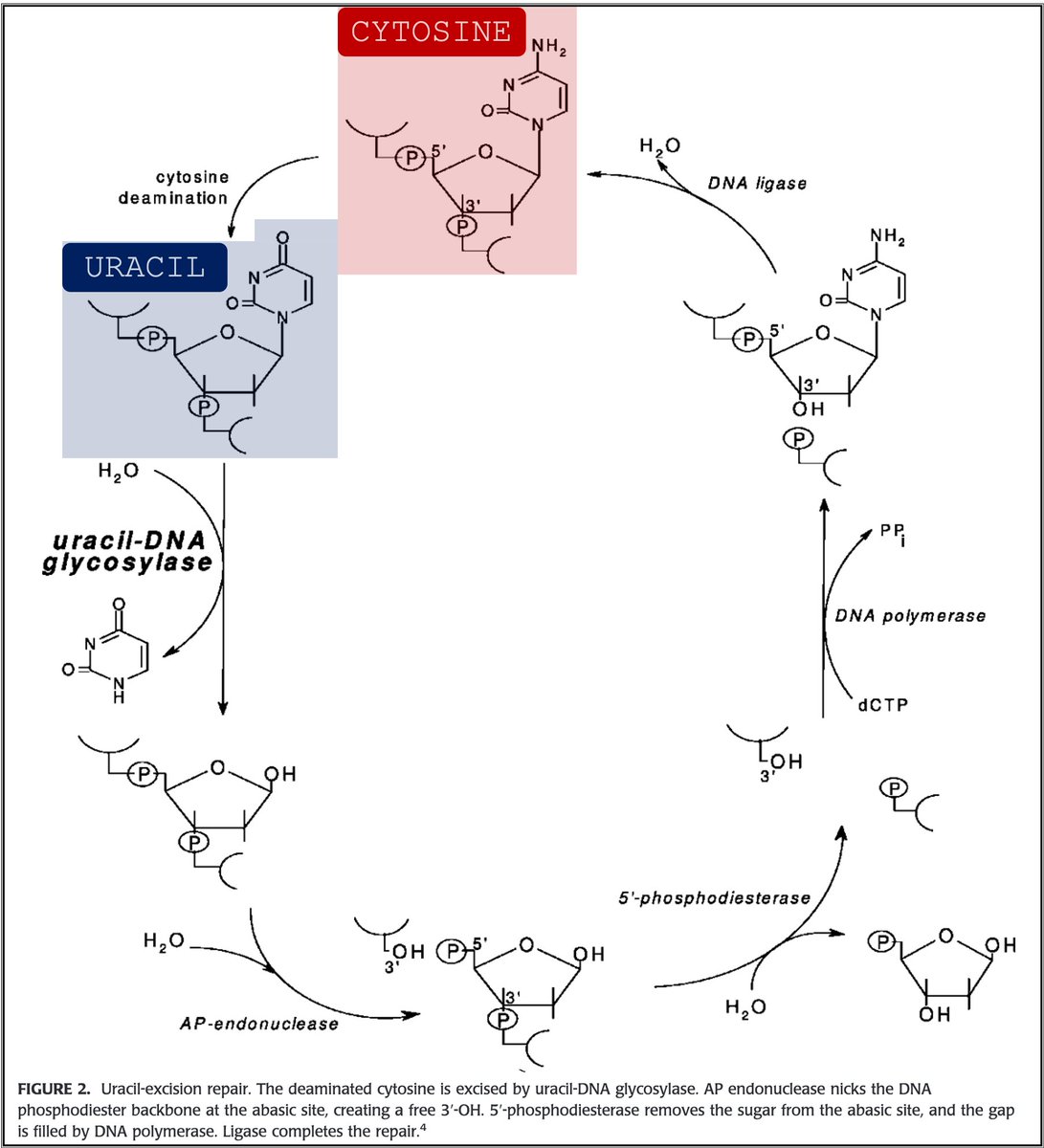
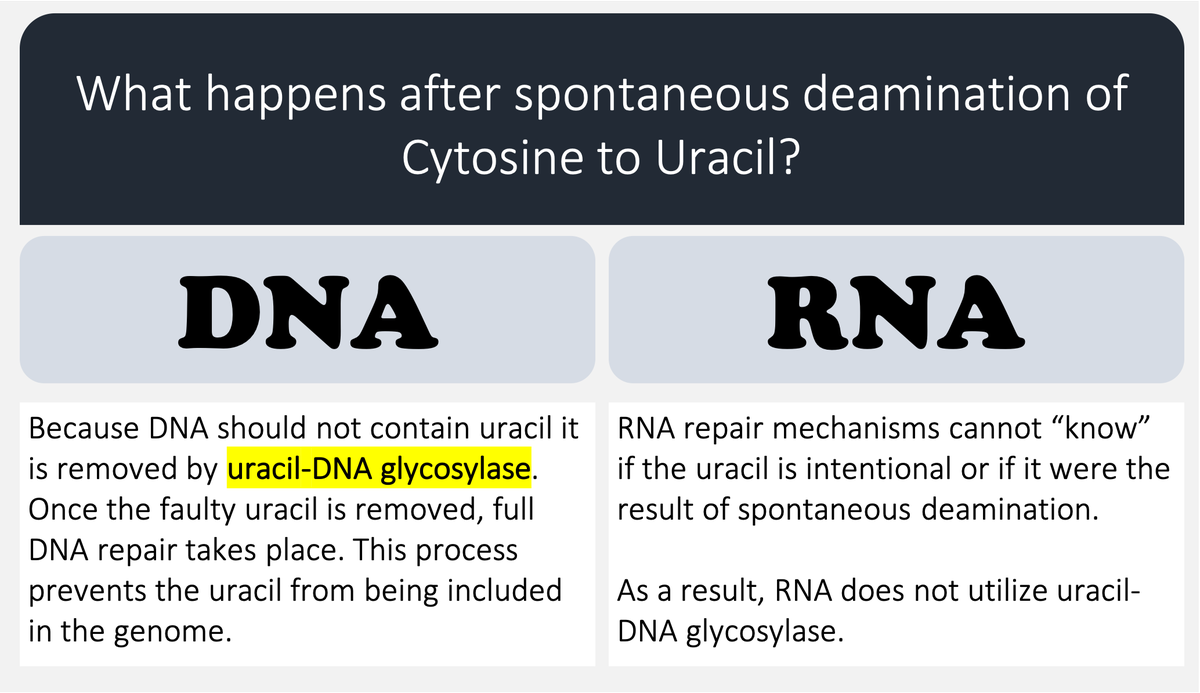
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
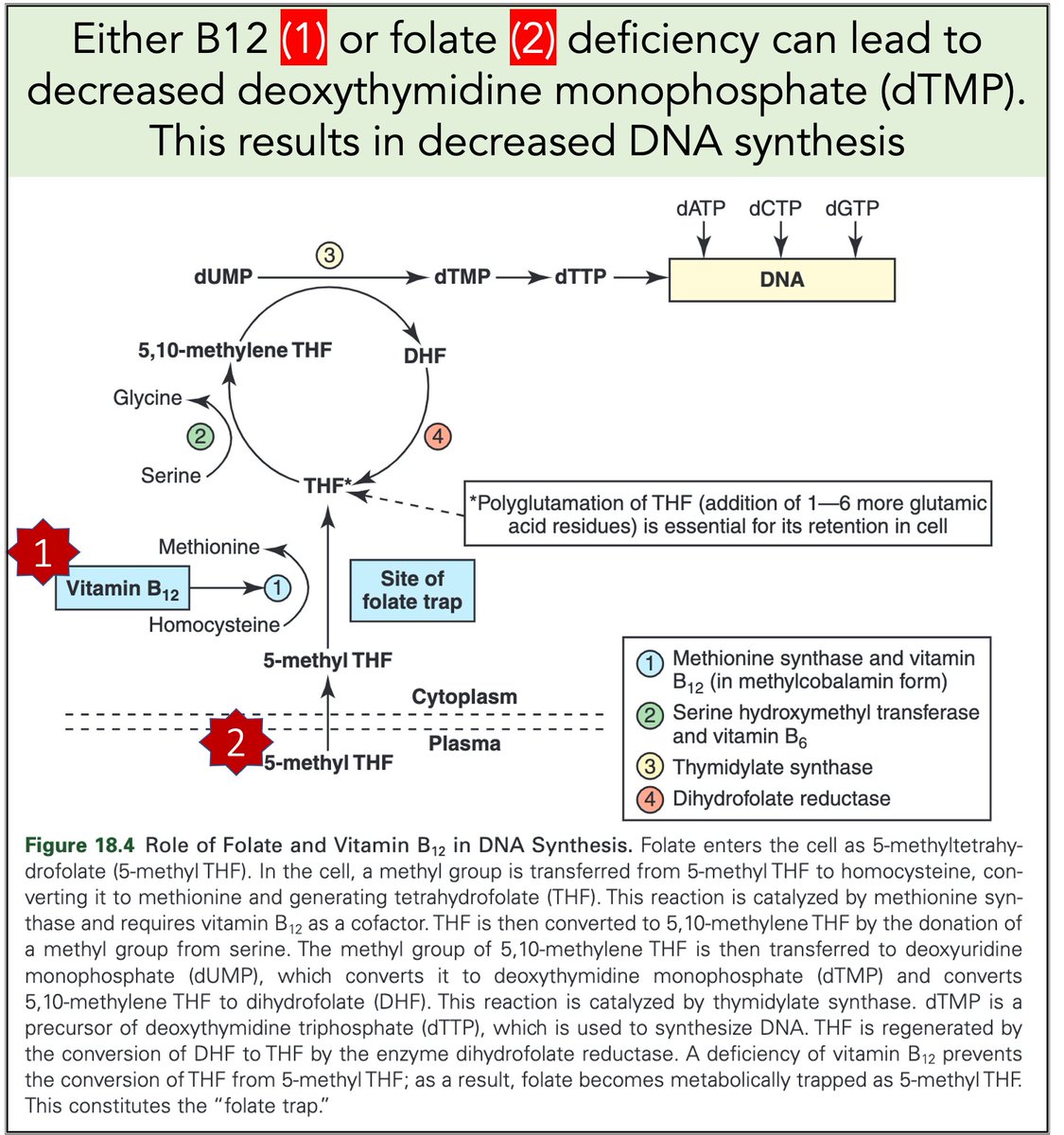
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh







Before we get too far into 2021, I thought I’d write a thread recapping some of the research that came out of my lab in 2020. Most of this work was led by my talented team of graduate students, Kerrianne Morrison, @kmdebrabander, and @DesiRJones.
Back in January, a news story was published about Kerrianne’s study showing improved social interaction outcomes for autistic adults when paired with another autistic partner.
A detailed thread about the study and a link to the paper can be found here (feel free to DM me your email address if you’d like a copy of the full paper for this study or any of our studies):
Another paper published early in 2020 (it appeared a few months earlier online) showed that traditional standalone tasks of social cognition are less predictive of functional and social skills among autistic adults than commonly assumed in autism research.
Next, @kmdebrabander led and published an innovative study about how well autistic and non-autistic adults can predict their own cognitive and social cognitive performance.
Back in January, a news story was published about Kerrianne’s study showing improved social interaction outcomes for autistic adults when paired with another autistic partner.
A detailed thread about the study and a link to the paper can be found here (feel free to DM me your email address if you’d like a copy of the full paper for this study or any of our studies):
In our new paper out today, autistic adults held a \u201cget to know you\u201d conversation with an unfamiliar autistic or typically-developing (TD) person. We were curious: would social interaction outcomes differ when their partner was also autistic? THREAD https://t.co/4koqUKV9G1
— Noah Sasson (@Noahsasson) December 11, 2019
Another paper published early in 2020 (it appeared a few months earlier online) showed that traditional standalone tasks of social cognition are less predictive of functional and social skills among autistic adults than commonly assumed in autism research.
How well does social cognition predict functional and social skills in autism? Our new paper attempts to answer this question. This thread summarizes why we conducted the study, what we found, and why I think it\u2019s important. https://t.co/KB1nIpK0M2
— Noah Sasson (@Noahsasson) August 16, 2019
Next, @kmdebrabander led and published an innovative study about how well autistic and non-autistic adults can predict their own cognitive and social cognitive performance.
New by @kmdebrabander and our lab: Autistic adults don\u2019t differ from non-autistic adults in the accuracy of their self-assessment on general cognitive tasks but are less accurate on social cognitive tasks. This however was unrelated to social functioning https://t.co/0MrqMKKO0r
— Noah Sasson (@Noahsasson) September 20, 2020

You gotta think about this one carefully!
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇
Imagine you go to the doctor and get tested for a rare disease (only 1 in 10,000 people get it.)
The test is 99% effective in detecting both sick and healthy people.
Your test comes back positive.
Are you really sick? Explain below 👇
The most complete answer from every reply so far is from Dr. Lena. Thanks for taking the time and going through
Really doesn\u2019t fit well in a tweet. pic.twitter.com/xN0pAyniFS
— Dr. Lena Sugar \U0001f3f3\ufe0f\u200d\U0001f308\U0001f1ea\U0001f1fa\U0001f1ef\U0001f1f5 (@_jvs) February 18, 2021
You can get the answer using Bayes' theorem, but let's try to come up with it in a different —maybe more intuitive— way.
👇
Here is what we know:
- Out of 10,000 people, 1 is sick
- Out of 100 sick people, 99 test positive
- Out of 100 healthy people, 99 test negative
Assuming 1 million people take the test (including you):
- 100 of them are sick
- 999,900 of them are healthy
👇
Let's now test both groups, starting with the 100 people sick:
▫️ 99 of them will be diagnosed (correctly) as sick (99%)
▫️ 1 of them is going to be diagnosed (incorrectly) as healthy (1%)
👇
You May Also Like


H was always unseen in S2NL :)
Those who exited at 1500 needed money. They can always come back near 969. Those who exited at 230 also needed money. They can come back near 95.
Those who sold L @ 660 can always come back at 360. Those who sold S last week can be back @ 301
Those who exited at 1500 needed money. They can always come back near 969. Those who exited at 230 also needed money. They can come back near 95.
Those who sold L @ 660 can always come back at 360. Those who sold S last week can be back @ 301
Sir, Log yahan.. 13 days patience nhi rakh sakte aur aap 2013 ki baat kar rahe ho. Even Aap Ready made portfolio banakar bhi de do to bhi wo 1 month me hi EXIT kar denge \U0001f602
— BhavinKhengarSuratGujarat (@IntradayWithBRK) September 19, 2021
Neuland 2700 se 1500 & Sequent 330 to 230 kya huwa.. 99% retailers/investors twitter par charcha n EXIT\U0001f602

A brief analysis and comparison of the CSS for Twitter's PWA vs Twitter's legacy desktop website. The difference is dramatic and I'll touch on some reasons why.
Legacy site *downloads* ~630 KB CSS per theme and writing direction.
6,769 rules
9,252 selectors
16.7k declarations
3,370 unique declarations
44 media queries
36 unique colors
50 unique background colors
46 unique font sizes
39 unique z-indices
https://t.co/qyl4Bt1i5x

PWA *incrementally generates* ~30 KB CSS that handles all themes and writing directions.
735 rules
740 selectors
757 declarations
730 unique declarations
0 media queries
11 unique colors
32 unique background colors
15 unique font sizes
7 unique z-indices
https://t.co/w7oNG5KUkJ

The legacy site's CSS is what happens when hundreds of people directly write CSS over many years. Specificity wars, redundancy, a house of cards that can't be fixed. The result is extremely inefficient and error-prone styling that punishes users and developers.
The PWA's CSS is generated on-demand by a JS framework that manages styles and outputs "atomic CSS". The framework can enforce strict constraints and perform optimisations, which is why the CSS is so much smaller and safer. Style conflicts and unbounded CSS growth are avoided.
Legacy site *downloads* ~630 KB CSS per theme and writing direction.
6,769 rules
9,252 selectors
16.7k declarations
3,370 unique declarations
44 media queries
36 unique colors
50 unique background colors
46 unique font sizes
39 unique z-indices
https://t.co/qyl4Bt1i5x
PWA *incrementally generates* ~30 KB CSS that handles all themes and writing directions.
735 rules
740 selectors
757 declarations
730 unique declarations
0 media queries
11 unique colors
32 unique background colors
15 unique font sizes
7 unique z-indices
https://t.co/w7oNG5KUkJ
The legacy site's CSS is what happens when hundreds of people directly write CSS over many years. Specificity wars, redundancy, a house of cards that can't be fixed. The result is extremely inefficient and error-prone styling that punishes users and developers.
The PWA's CSS is generated on-demand by a JS framework that manages styles and outputs "atomic CSS". The framework can enforce strict constraints and perform optimisations, which is why the CSS is so much smaller and safer. Style conflicts and unbounded CSS growth are avoided.

1/12
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
4/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
...indication, first of all that testing for a (single) respiratory virus is done outside of surveillance systems or need for specific therapy, but even so the lack of consideration of Ct, symptoms and clinical findings when interpreting its result. https://t.co/gHH6kwRdZG
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
6/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
The neither validated nor standardised hypersensitive RT-PCR test / Ct 35-45 for SARS-CoV-2 is abused to mislabel (also) other diseases, especially influenza, as COVID-19.https://t.co/AkFIfTCTkS
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.https://t.co/mbNY8bdw1p pic.twitter.com/OQBD4grMth
— Dr. Thomas Binder, MD (@Thomas_Binder) November 29, 2020
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
Thread web\u2b06\ufe0f\u2b07\ufe0f
— Dr. Thomas Binder, MD (@Thomas_Binder) December 16, 2020
The fabrication of the "asymptomatic (super) spreader" is the coronation of the total nons(ci)ense in the belief system of #CoronasWitnesses.
Asymptomatic transmission 0.7%; 95% CI 0%-4.9% - could well be 0%!https://t.co/VeZTzxXfvT
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
8/8
— Dr. Thomas Binder, MD (@Thomas_Binder) March 24, 2020
By the way, who the f*** created this obviously (almost) worldwide definition of #CoronaDeath?
This is not only medical malpractice, this is utterly insane!https://t.co/FFsTx4L2mw

