The pre CISION tech is simply an attempt to improve the safety profile... 2/10
AVA6000 approved by MHRA. Superb news. First dosing 'around mid-year'; first data to come within 3-4 months after that.
A summary thread on the significance of AVA6000 - and #AVCT's pre CISION platform as a whole - to both the oncology industry and to AVCT itself. 1/10
The pre CISION tech is simply an attempt to improve the safety profile... 2/10
Most therapeutics going through clinical trials look for an improvement of at least 20% over the existing industry-standard drug. A 50% increase in efficacy would usually be considered an astonishing result.
In pre-clinical mouse models for #AVCT's AVA6000 3/10
What this means is that the pre CISION tech could be used to enable the giving of doses to patients that are multiple times more potent... 4/10
For example, in #AVCT's pre-clinical trials, pro-dox (AVA6000) doses were 6x more potent than the standard dox doses.
The results? The...5/10
#AVCT isn't looking to improve chemotherapies by 25-30%, like most drugs in clinical trials.
Its pre CISION has the potential to improve the safety profile - and thus the... 6/10
https://t.co/XOEE45CBtZ
AVCT holds the global exclusive licence over...8/10
TMAC will produce Affimer Drug Conjugates - a potentially more powerful class of oncology treatment than Antibody Drug Conjugates. 9/10
First though, success for AVA6000 please!
Then hopefully @avacta's first TMAC drug to enter Phase I next year 10/10
More from Society





I've seen many news articles cite that "the UK variant could be the dominant strain by March". This is emphasized by @CDCDirector.
While this will likely to be the case, this should not be an automatic cause for concern. Cases could still remain contained.
Here's how: 🧵
One of @CDCgov's own models has tracked the true decline in cases quite accurately thus far.
Their projection shows that the B.1.1.7 variant will become the dominant variant in March. But interestingly... there's no fourth wave. Cases simply level out:
https://t.co/tDce0MwO61
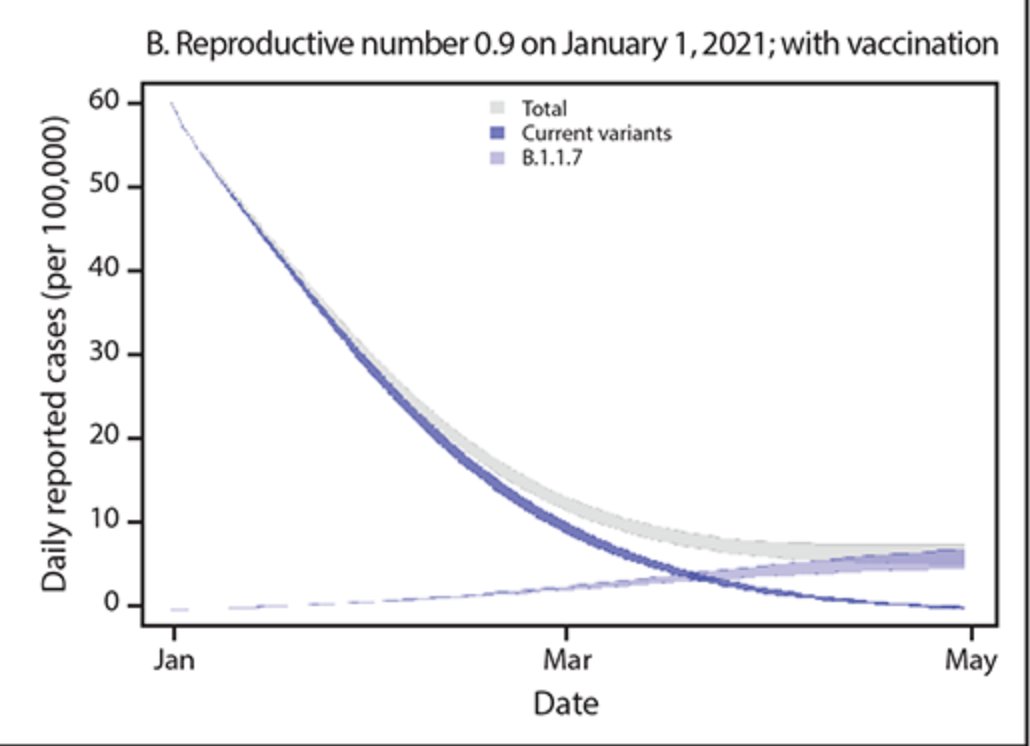
Just because a variant becomes the dominant strain does not automatically mean we will see a repeat of Fall 2020.
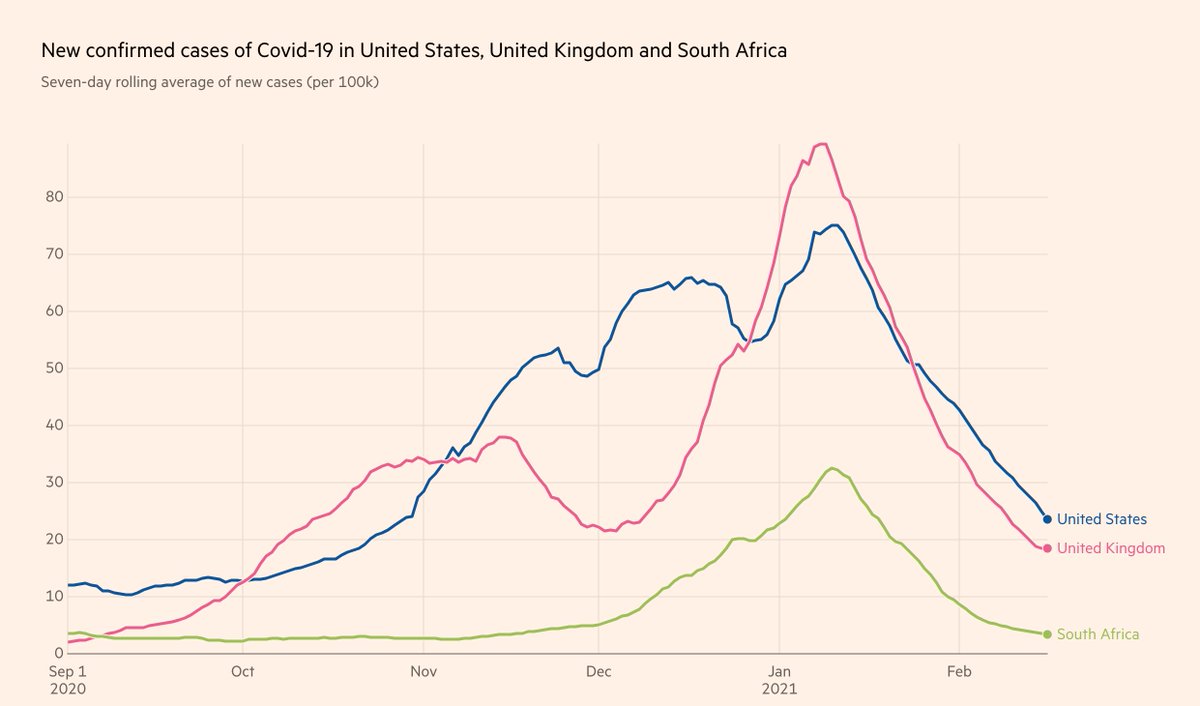
Let's look at UK and South Africa, where cases have been falling for the past month, in unison with the US (albeit with tougher restrictions):
Furthermore, the claim that the "variant is doubling every 10 days" is false. It's the *proportion of the variant* that is doubling every 10 days.
If overall prevalence drops during the studied time period, the true doubling time of the variant is actually much longer 10 days.
Simple example:
Day 0: 10 variant / 100 cases -> 10% variant
Day 10: 15 variant / 75 cases -> 20% variant
Day 20: 20 variant / 50 cases -> 40% variant
1) Proportion of variant doubles every 10 days
2) Doubling time of variant is actually 20 days
3) Total cases still drop by 50%
While this will likely to be the case, this should not be an automatic cause for concern. Cases could still remain contained.
Here's how: 🧵
One of @CDCgov's own models has tracked the true decline in cases quite accurately thus far.
Their projection shows that the B.1.1.7 variant will become the dominant variant in March. But interestingly... there's no fourth wave. Cases simply level out:
https://t.co/tDce0MwO61
Just because a variant becomes the dominant strain does not automatically mean we will see a repeat of Fall 2020.
Let's look at UK and South Africa, where cases have been falling for the past month, in unison with the US (albeit with tougher restrictions):
Furthermore, the claim that the "variant is doubling every 10 days" is false. It's the *proportion of the variant* that is doubling every 10 days.
If overall prevalence drops during the studied time period, the true doubling time of the variant is actually much longer 10 days.
Simple example:
Day 0: 10 variant / 100 cases -> 10% variant
Day 10: 15 variant / 75 cases -> 20% variant
Day 20: 20 variant / 50 cases -> 40% variant
1) Proportion of variant doubles every 10 days
2) Doubling time of variant is actually 20 days
3) Total cases still drop by 50%